
|
||||||||||||||||||||||||||||||||||||||||||||||||
|
NEUROANATOMIE CHIRURGICALE / SURGICAL NEUROANATOMY
EVALUATION OF THE CLINICO-ANATOMICAL RELATIONSHIPS BETWEEN ONODI CELLS, OPTIC NERVE, AND THE SPHENOID SINUS, USING TOMOGRAPHIC IMAGING.
ÉVALUATION DES RELATIONS CLINICO-ANATOMIQUES ENTRE LES CELLULES D'ONODI, LE NERF OPTIQUE ET LE SINUS SPHENOÏDE, A L'AIDE DE L'IMAGERIE TOMOGRAPHIQUE
E-Mail Contact - ALIU Abdulhameed :
aliu.abdulhameed@udusok.edu.ng
ABSTRACT Background: Accidental injury to the optic nerve during endoscopic transsphenoidal skull base interventions, resulting in permanent visual loss, can be frustrating. The chances of this injury increases with the presence of Onodi cells. In order to prevent or control these complications, a pre-interventional computed tomography (CT) assessment of the sphenoid sinus anatomy, for the identification of Onodi cells and its relationship with the optic nerve is essential. The aim of this study was to determine the prevalence of Onodi cells among adults of African (Nigerian) descent, and to assess its relationships with the optic nerve using CT. Methods: A retrospective, descriptive and analytical study was carried out on 323 CT slides of sphenoid sinus of adults (18 – 80 years), taken over a five year period (November 2014 and October 2019), for the analysis of Onodi cells. Results: The prevalence of Onodi cells was 4.0%, and were more frequently found among males (2.5%), than females (1.5%). Dehiscence of the optic canal and pneumatisation of the anterior clinoid process occurred in 7.74% and 20.12%, respectively. There was a statistically significant association between the presence of Onodi cells and age groups (X2 = 0.015), and the anterioposterior sinus diameter (X2 = 0.019), respectively. Conclusion: From this study, the prevalence of Onodi cells was fortunately low in comparison with values from other studies. A prospective study with rationalized CT protocols for identifying Onodi cells and its relationship with the optic nerve is suggested. Keywords: Computed Tomography, Onodi cells, Prevalence, Sphenoid Sinus. RESUME Contexte: Une lésion accidentelle du nerf optique lors d’interventions endoscopiques transsphénoïdiennes à la base du crâne, entraînant une perte visuelle permanente, peut être frustrante. Les risques de cette blessure augmentent avec la présence de cellules d’Onodi. Afin de prévenir ou de contrôler ces complications, une évaluation par tomodensitométrie pré-interventionnelle de l’anatomie du sinus sphénoïde, pour l’identification des cellules d’Onodi et sa relation avec le nerf optique est essentielle. Le but de cette étude était de déterminer la prévalence des cellules d’Onodi chez les adultes d’origine africaine (nigériane) et d’évaluer ses relations avec le nerf optique à l’aide du scanner. Méthodes: Une étude rétrospective, descriptive et analytique a été réalisée sur 323 coupes scannographiques de sinus sphénoïde d’adultes (18 – 80 ans), receuillies sur une période de cinq ans (novembre 2014 et octobre 2019), pour l’analyse des cellules d’Onodi. Résultats: La prévalence des cellules d’Onodi était de 4,0% et était plus fréquente chez les hommes (2,5%) que chez les femmes (1,5%). La déhiscence du canal optique et la pneumatisation du processus clinoïde antérieur sont survenues respectivement dans 7,74% et 20,12%. Il y avait une association statistiquement significative entre la présence de cellules d’Onodi et les groupes d’âge (X2 = 0,015) et le diamètre du sinus antéro-postérieur (X2 = 0,019), respectivement. Conclusion: D’après cette étude, la prévalence des cellules d’Onodi était heureusement faible par rapport aux valeurs d’autres études. Une étude prospective avec des protocoles scanner rationalisés pour identifier les cellules d’Onodi et sa relation avec le nerf optique est suggérée. Mots-clés: tomodensitométrie, cellules d’Onodi, prévalence, sinus sphénoïde. INTRODUCTION: Onodi (sphenoethmoidal) cells are described as variants of the most posterior ethmoidal cells, which pneumatises superiolateral to the sphenoid sinus. Named after the Hungarian rhinolaryngologist, Adolf Onodi, they lie intimately related to the optic canal, and may extend into the anterior clinoid processes (9,10.13,22). The endoscopic endonasal transsphenoidal approach to the base of the skull is now widely being employed in the management of diseases affecting structures in the vicinity of the sphenoid sinus, such as, optic nerve decompression and pituitary hypophysectomy. This is because, this route is quicker, safer, and a direct access to the sphenoid, with better visualisation, that allows a more complete removal of a pituitary adenoma (28). However, during this procedure, an unidentified Onodi cell, within the field of operation, or a dehiscent wall of the optic canal, increases the risk of inadvertent injury to the optic nerve (21). With the resultant complication of blindness, patient’s life could become frustrating with hopelessness. The use of computerized tomography (CT), as an investigative tool, has improved the quality and quantity of available information, derivable from the assessment of the paranasal sinuses, which are not directly visible using other radiologic procedures like the X-ray (3,32). Therefore, in order to prevent or control these complications, pre-interventional CT assessment of the sphenoid sinus anatomy, Onodi cells, if present, and its relationship with the optic nerve, is essential for a safe endoscopic transsphenoidal procedure. The prevalence of Onodi cells was 13% each, (11,24), in a study of 30 cadavers, and among 100 Sudanese subjects, although very low prevalence of 5% has been reported (12). Similarly, other studies have identified higher Onodi cell incidences; 18% in 100 subjects (18), and 30.6% among 350 Chinese subjects (17). In Nigeria, and Africa, there is a general paucity of data on the prevalence of Onodi cells using CT. As such, the aim of this study was to determine the prevalence of Onodi cells, and assess their relationships with the optic nerve by means of computerised tomography. We have also reported the prevalence of dehiscence of the optic canal and pneumatisation of the anterior clinoid process, due to their relationship to Onodi cells, when present, and their common ability to increase the chances of injury to the optic nerve during surgery. MATERIALS AND METHODS: Three hundred and twenty three adult sphenoid sinuses, obtained from individuals with age, ranging from 18 to 80 years, (mean age, 41.4 years ± 17.8), were retrospectively studied at the Radiology Department of the Usmanu Danfodiyo University Teaching Hospital, Sokoto, following institutional ethical approval. CT images with evidence of sinus disease, surgery, craniofacial anomalies or tumors distorting the normal anatomy of the skull base and sphenoethmoidal region were excluded. All images were taken between November 2014 and October 2019, using a GE Bright Speed Multidetector Helical CT (GE Healthcare, U.S.A, 2005) Scanner, at 200 mAs, 120 KVp, 15 cm Field of View, slice thickness of 2.5 mm, 512 X 512 matrix and a standard reconstruction algorithm. The CT slides were viewed on the computer using the Digital Imaging and Communication in Medicine (DICOM, Poland) viewer, powered by the RadiAnt Version 4.2 software. Onodi cells were studied and identified on axial and coronal reconstructed images, as aerated cavities on the superiolateral aspects of the body of the sphenoid sinus, either unilateral or bilateral, and noted to occasionally extend into the anterior clinoid processes (2,16) (Figure 1 and 2). Pneumatisation of the anterior clinoid process and dehiscence of the bony walls of the optic nerve were also studied on similar planes. Three dimensions (the anteroposterior (AP), craniocaudal (CC), and transverse (TR), diameters), of the sphenoid sinus were measured on sagittal reformatted, axial and coronal reconstructed CT images, while the volume was calculated, using the ellipsoid formula; Sinus Volume = 4/3 x π x A x B x C/23 (1), where, A, B, and C are the ellipsoid diameters corresponding to AP, CC, and TR diameters respectively. Data was tabulated and entered into computer using Microsoft Excel. SPSS Version 22 was used for data analysis. Statistical tests were employed for data analysis. Comparison of mean values of measured parameters in relation to sex and age distribution of the subjects were carried out using one way analysis of variance (ANOVA), while proportions were compared using chi-square test. Logistic regression was carried out to test for association between the presence of Onodi cells and age, sex, and dimensions of the sphenoid sinus. RESULTS: Prevalence of Onodi cells in the population From this study, the prevalence of Onodi cells was 4.0% (13 subjects). 0.9% (3 subjects) were unilateral, while, 3.1% (10 subjects) were bilateral (Figure 3). Prevalence of optic nerve dehiscence and pneumatisation of the anterior clinoid process The prevalence of optic nerve dehiscence from this study was 7.74% (25 subjects). This occurrence was more frequently bilateral (3.71%), than located on either right or left sides (Table 1). Pneumatisation of the anterior clinoid process occurred in 20.12% (65 subjects), and this incidence was also frequently bilateral (13.00%) (Table 1). In Figure 3, females had higher prevalence of both bilateral and overall incidence of optic nerve dehiscence and pneumatisation of the anterior clinoid process respectively. Relationship between age/sex and Onodi cells There was a statistically significant relation between the presence of Onodi cells and age of subjects (p = 0.015), (Table 2). Onodi cells were more frequently found among males (8 subjects; 2.5% ; 2 unilateral and 6 bilateral), than in females (5 subjects; 1.5%, 1 unilateral, and 4 bilateral) (Figure 3). However, there was no statistically significant relationship between the presence of Onodi cells and sex of subjects (p = 0.282) (Table 1). Logistic regression: Test of association between sinus dimensions, age and sex, and the presence of Onodi cells From this study, there was a statistically significant association between the anteroposterior diameter (length) of the sphenoid sinus and the presence of Onodi cells (Table 2). Interestingly, there was no statistically significant association between the degree of pneumatisation of the sphenoid sinus and the occurrence of Onodi cell (Table 2). DISCUSSION Onodi cells are embryologically derived from ethmoidal cells. They however, undergo differentiation to become intricately related to the anterior and superior-lateral aspects of the sphenoid sinus, the optic nerve, and internal carotid artery (29). The occurrence of optic neuropathy from pathological processes in Onodi cells is an indication of the intimacy between it and the optic nerve, as the nerve is frequently found running within the small cavity of the Onodi cell (16). Knowledge of the presence of an Onodi cell is key to prevent inadvertent injury to the optic nerve during endoscopic sinus and skull base surgeries (29,30). Notwithstanding, Onodi cells could give rise to isolated mucoceles, that consequently compress the optic nerve resulting in acute onset of visual loss (14,15,31). According to Driben (6), Onodi cells are more common anatomical variants of the sphenoid sinus than previously appreciated, and the incidence ranges from 8% to 14% (9,11,24,27,30). However, higher prevalence of 18% has been reported in Romania (18), 30.6% among Chinese subjects (17), 49.5% (13), and 65.3% (29). A prevalence of 5% was reported among Indians (12), however, among Nigerians in the southwest, Onodi cells occurred in 18.4% of subjects (7). Our study found a prevalence of 4%; this is lower than the results of these previous studies, despite the relatively higher number of our sample size. The differences may be due to the fact that, a number of these previous studies were conducted on cadavers with a relatively small number of patients (3,28), and others were carried out by endoscopic examination (25). The differences in the slide thickness, environmental, genetic and racial factors may have contributed to the differences between these studies. With the several CT protocols for identifying and defining Onodi cells (15), some studies have suggested that a combination of CT assessment and transnasal endoscopic examination would be necessary to avoid missed Onodi cells on CT (6,25). With the low prevalence of Onodi cells in this study, we think, it may be important to apply this combination of methods, to ensure that, a satisfactory and accurate prevalence for Onodi cell in the population is achieved. Pneumatisation of the anterior clinoid process and dehiscence of the optic canal are normal variations of the complex anatomy of the sphenoid sinus. Identifying them is critical, to minimize surgical risks and decrease morbidity (17,29). The pneumatisation of the anterior clinoid process could extend, such that, its edges fuse and blends with the walls of the sphenoid sinus. This would obscure the landmark it provides duces in its relationship with the optic nerve, which now become exposed within the sinus (17). In addition, dehiscence of the optic canal gives rise to bulging, such that, a whole, or part of the optic nerve becomes bare and unprotected (29). These conditions lead to optic nerve protrusion into the super-lateral aspect of the sphenoid sinus, thus, increasing its risks of inadvertent surgical injury (17). In this study, pneumatisation of the anterior clinoid process occurred in 20.12% (65 subjects); this is higher than the 10%, among 350 Chinese subjects (17), and the 9.2% in 300 Japanese patients (19). However, other studies have shown that, the prevalence of pneumatisation of the anterior clinoid process could range from 4 to 29.3% (4,5,23,26). The prevalence of optic nerve dehiscence from this study was 7.74% (25 subjects). This is higher than the 4%, in 25 dissected cadavers in Florida (8), 5%, among 200 Romanian subjects (18), 1.8%, and 1.5%, among Hispanics and African Americans respectively (29), but similar to the prevalence 7.7%, among Asians, and 7.4%, among Caucasians (29). The wide differences in the sample sizes, methodology (dissection/CT), racial, environmental and genetic factors may have contributed to the differences observed in these results. The statistically significant relationship between age and presence of Onodi cell, from this study reveals that, with advancing age, the chances of identifying an Onodi cell on CT increases. However, this was not the case with sex of subjects. CONCLUSION: The prevalence of Onodi cell among a population of north-western Nigeria was low. Increasing age of subjects and the anterioposterior diameter of the sphenoid sinus were associated with the presence of Onodi cells. An adequate pre-interventional method of identification and confirmation of the presence of Onodi cell is the key for a safe endoscopic sinus surgery. Acknowledgment: We acknowledge the department of Radiology, Usmanu Danfodiyo University Sokoto. Conflict of interest: The authors declare no conflicts of interest
Table 1. Prevalence and location of optic nerve dehiscence and pneumatisation of the anterior clinoid process
Table 2: Test of association between the presence of Onodi cells and features of the sphenoid sinus
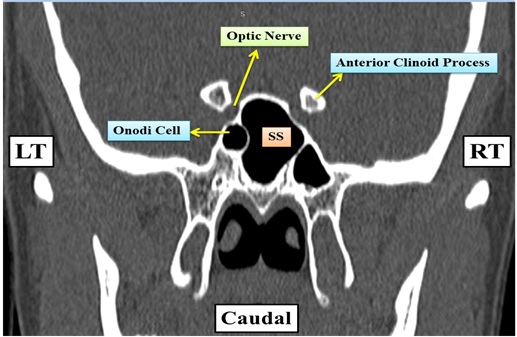
Figure 1: Coronal CT of sphenoid sinus of a 68 year old male showing a left sided Onodi cell and its relation to the left optic nerve. SS = Spenoid Sinus cavity, RT = Right Side, LT = Left Si
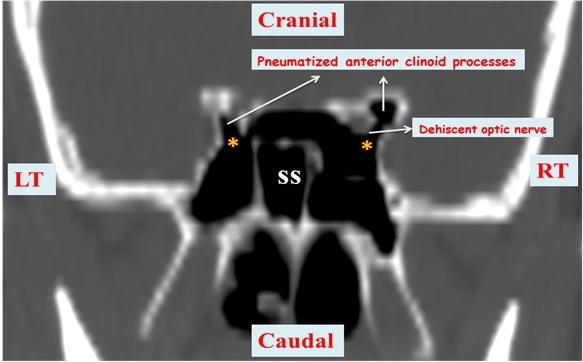
Figure 2: Coronal CT of sphenoid sinus of a 52 year old male showing bilateral Onodi cells (marked ⃰), a dehiscent right optic nerve, and bilaterally pneumatised anterior clinoid processes just lateral to the optic canal. SS = Spenoid Sinus cavity, RT = Right Side, LT = Left Si
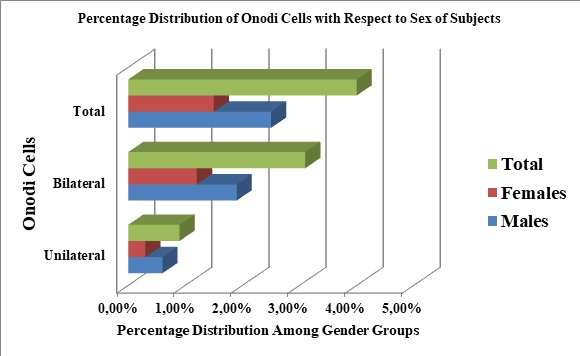 Figure 3: Prevalence of Onodi cells in the studied population
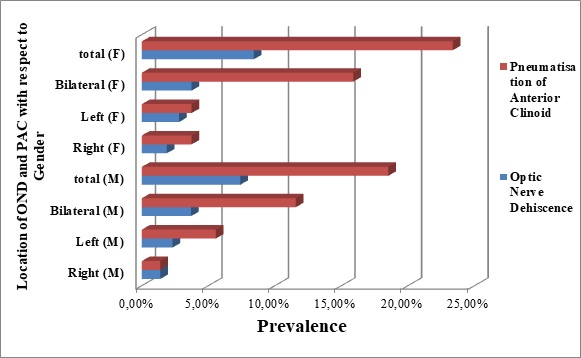 Figure 4: A 3-D bar chart, showing the locations (sides) and prevalence of optic nerve dehiscence (OND), and pneumatisation of the anterior clinoid process (PAC), among the genders (male = M, female = F). REFERENCES
|
||||||||||||||||||||||||||||||||||||||||||||||||
© 2002-2018 African Journal of Neurological Sciences.
All rights reserved. Terms of use.
Tous droits réservés. Termes d'Utilisation.
ISSN: 1992-2647