
|
|
|
CASE REPORT / CAS CLINIQUE
LIPIDISED FAUX MENINGIOMA: CASE REPORT
MÉNINGIOME LIPOMATEUX DE LA FAUX : CAS CLINIQUE
E-Mail Contact - ULIVIERI Simone :
simone.ulivieri@tiscali.it
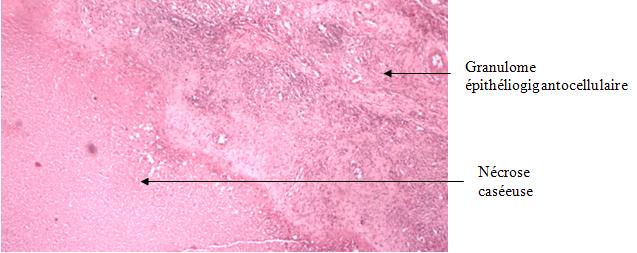
ABSTRACT Variously referred to a lipomatous meningioma, lipidised meningioma or lipomeningioma, this benign meningothelial tumour represents 0.3% of all meningioma. RESUME Le lipoméningiome est une tumeur méningotheliale bénigne et représente 0.3% des méningiomes. Approximativement 50 cas de lipoméningiome ont été trouvés dans la littérature. Nous décrivons un cas de lipomeningiome histologiquement confirmé et discutons la pathologie avec sa présentation clinique. Key words: falx-immunohistochemistrty-lipomeningioma INTRODUCTION Lipidised meningioma was first reported by Bailey and Bucy in 1931 (1 ).In the 2000 World Health Organization Classification of Tumors of the Nervous System, meningiomas with lipomatous changes are classified as metaplastic meningiomas, as are meningioma with osseous, cartilaginous, myxoid and xanthomatous changes. These tumours mostly occur in the parietal and frontal convexity and exceptionally in the skull base and spine (2, 6). CASE REPORT A 61-year-old woman presented with a history of headache of a few months duration. On admission the neurological examination revealed no neurological deficits. MRI study showed an extra-axial lesion of the flax cerebri, 2.3 cm in diameter, that was hyper-intense on T1 and T2 -weighted images and decreased intensity on fat suppressed sequences (Fig 1). The patient underwent a left fronto-parietal craniotomy and interhemisferic approach. A durally based tumour with fat content was coagulated and excised, noted to not involve the brain; histopathological examinations revealed the characteristic appearance of a meningioma composed of mature adipose tissue (Fig.2). The proportion of lipid content was about 60 %. There was no xanthomatous area, no atypical features, no lipoblastlike and immunohistochemically the meningothelial and lipomatous foci was positive for vimentin and epithelial membrane antigen and negative for S-100 only the first one. The postoperative course was uneventful without any complications and was discharged eight days after the operation. MRI exam performed 6 months later revealed no signs of recurrence. DISCUSSION Meningioma is a common tumor that constitutes approximately 20% of all primary brain tumors. Lipidised histological type is well described but certainly uncommon. Radiologically it appears hypodense on CT and shows high intensity on T1-weighted ant T2- weighted MRI and the high intensity area on T1-weighted MRI is changed to a low intensity area on fat suppressed T1-weighted imaging and differential radiographic diagnosis is between lipoma, teratoma and meningioma. Histogically this tumor presents as whorl formations of meningothelial cells with only one triglyceride droplet and a maldistributed nucleus (4) and usually the proportion of lipid content is extremely variable from 10 to 90 % (3).Electron microscopy showed cytoplasmic intermediate filaments, interdigitating cell processes and well-formed desmosomes in the lipomatous foci as are seen in conventional meningothelial foci. Based on the immunohistochemical findings Roncaroli (5) suggested that these neoplastic cells should not be considered true metaplasia but a metabolic abnormality of the neoplastic cells and that lipidised meningioma is the more appropriate term. Clinical features and prognosis of this rare histological tumor are not different from those of usual meningioma and surgical strategy has to be always valued and often used.  Figure 1  Figure 2
REFERENCES
|

© 2002-2018 African Journal of Neurological Sciences.
All rights reserved. Terms of use.
Tous droits réservés. Termes d'Utilisation.
ISSN: 1992-2647