
|
|
|
CASE REPORT / CAS CLINIQUE
LONG TERM FOLLOW UP OF A PATIENT WITH AN ECTOPIC PROLACTINOMA MIMICKING A CLIVAL CHORDOMA
SUIVI A LONG TERME D'UN PATIENT PRESENTANT UN PROLACTINOME ECTOPIQUE IMITANT UN CHORDOME DU CLIVUS
E-Mail Contact - NAIDOO Dinesh :
dineshnaidoo@yahoo.com
ABSTRACT This is a short report of a patient initially thought to have a clival chordoma. The lesion was, and continues to be, successfully medically treated as a prolactinoma, approximately 11 years after the initial diagnosis. Key Words : Chordoma, Clivus, Ectopic, Prolactinoma RESUME Il s’agit d’une observation brève d un patient soupçonné initialement d’avoir un chordome du clivus. La lésion a été et continue d’être traitée avec succès comme un prolactinome, environ 11 ans après le diagnostic initial. Mots clés : Chordome, Clivus, Ectopique, Prolactinome CASE REPORT The patient is a 58-year-old male who presented in 2008 with a 2-day history of intermittent diplopia and decreased visual acuity, but no significant headache. He reported neither recent weight gain nor weight loss and neither heat nor cold intolerance. The patient did not report any nipple discharge. He was a known hypertensive on treatment but was otherwise previously well. Physical examination demonstrated normal visual acuity and normal visual fields. The appearances of both fundi were normal. The patient had a right abducens nerve palsy. He did not have galactorrhoea. CT scan demonstrated an erosive and expansile mass of the clivus. There was no expansion of the sella turcica and no mass within the sella. A subsequent MRI of the brain demonstrated a mixed signal, intensely enhancing mass within the clivus and an irregular clival contour. There was no soft tissue mass within an empty appearing sella turcica. The optic chiasm and pituitary stalk appeared normal with neither distortion nor displacement. The patient’s serum prolactin level was > 4000ng/dl. The serum levels of the remainder of the routinely tested pituitary hormone were normal. Bromocriptine, in the form of Parludel®, was commenced. Surgical intervention was not recommended. The commencement of anti-dopaminergic medication was followed by rapid resolution of the abducens nerve palsy and normalization of the prolactin level. Any attempt at stopping the bromocriptine resulted in markedly increased prolactin levels and the current treatment plan is to continue bromocriptine for life. The patient remains well, eleven years on, except for a recent diagnosis of glaucoma. The most recent MRI (February 2019) shows persistence of the empty sella appearance but no discernable clival mass. DISCUSSION Purely ectopic pituitary tumours are rare and were first described in 1909 by Erdheim (1, 2). It is much more common for a primary pituitary tumour, when aggressive, to invade adjacent structures such as the sphenoid sinus, cavernous sinuses, suprasellar region and, very rarely, the clivus. Clival tumours are very rare and comprise 1% of all intracranial neoplasms ( 8).The commonest tumours arising from the clivus are chordomas, chondrosarcomas, metastases and osteosarcomas (11) .Chordomas, originating from the clival synchondrosis, are the most common tumour of the clivus, accounting for about 40 percent of cases of primary clival tumours (2). CT scan and MRI findings of an expansile, destructive, lytic clival lesion with an associated soft tissue component are characteristic of chordomas. Chordomas can sometimes mimic pituitary adenomas if they have sella or parasellar extension. Progression free survival rates for chordomas are generally 50 percent or less (3). For chordomas radical resection is the treatment of choice (6). This, however, can only be done in about 50 percent of patients in highly specialized centers given the deep-seated location of the tumour and its proximity to vital neural and vascular structures (3, 6, 7). Patients with chordomas present with headache and a sixth nerve palsy most commonly. Thus, an initial diagnosis of a clival chordoma in this patient seemed radiologically and clinically appropriate. Prolactinoma and other pituitary tumours, ectopic or not, are rarely associated with destruction of the bony skull. Purely clival ectopic pituitary adenomas with no involvement of the pituitary gland are exceedingly rare (6). Ectopic pituitary tumours located in the clivus have been previously reported either isolated or in association with a pituitary tumour. An English literature review performed in December 2015 found that 17 cases of clival ectopic pituitary adenomas had been reported up to that date with no gender variance (8). The majority of these ectopic clival pituitary tumours were prolactinomas [10 out of 17]. A large number of cases [13 out of 17] could be diagnosed preoperatively. Varma et al reported a case of an ectopic clival prolactinoma in 2016 (12). The current case is, to the author’s knowledge, the first locally reported case of an ectopic clival pituitary adenoma, without sella involvement. Invasion of the cavernous sinuses and carotid arteries is rare and was reported only once. (8). Ectopic clival pituitary adenomas, particularly, prolactinomas appear to have an association with an empty sella turcica (5). A serum prolactin level of greater than 500 ng/dl is considered diagnostic of a macroprolactinoma (9), and where such a high level is found, treatment, if indicated, can be commenced without biopsy. The efficacy of treatment can be determined with serial serum prolactin levels in association with repeated imaging studies. Aggressive pituitary tumours with erosion of the skull base may be distinguished from chordomas preoperatively by clear sella involvement; and marked hyperprolactinemia in the case of aggressive prolactinomas. Such distinction, however, may at times only be made surgically and histologically. CONCLUSION Although exceedingly rare, the author concurs with Anand (1), that the differential diagnosis of a clival mass must always include an ectopic pituitary mass. Karras et el undertook partial resection of a clival mass which turned out to be an ectopic prolactinoma (8). It is their belief that proper consideration of this diagnosis could have avoided surgery in that instance. De Witte el al and Rocque et al similarly operated on a clival tumours,with no connection to the pituitary, which proved to be an ectopic prolactinomas (4,10).The consideration (and biochemical confirmation) of this diagnosis in the current case completely avoided the need for surgery and the patient remains well and symptom free more than 11 years later. 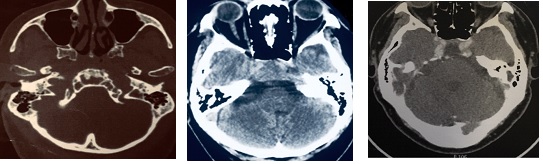 Figures 1,2,3. Initial axial CT scans showing expansion and destruction of the clivus, clival mass and absence of sella involvement. 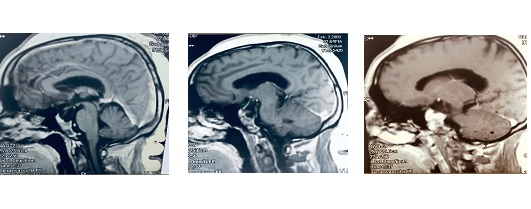 Figures 4,5,6 .Early sagittal and parsagittal contrasted MRI’s showing a lobulated tissue mass within the clivus with empty appearing sella turcica.  Figure 7. Early MRI showing normal appearance of pituitary stalk and optic chiasm and absence of sella tissue.  Figure 8. MRI 11 years after initial diagnosis showing normal appearing clivus with persistence of empty sella.
REFERENCES
|
© 2002-2018 African Journal of Neurological Sciences.
All rights reserved. Terms of use.
Tous droits réservés. Termes d'Utilisation.
ISSN: 1992-2647