TECHNIQUES
RECORDING EEG IN YOUNG CHILDREN WITHOUT SEDATION
PRATIQUE DE L'EEG CHEZ L'ENFANT SANS SEDATION
- Departamento de Neurofisiología, Centro Internacional de Restauración Neurológica. Ciudad de la Habana, CUBA
ABSTRACT
Background
Although it has been considered that sedation in children undergoing EEG tests is effective and safe and complications are infrequent, occasionally adverse sedation-related events are presented.
Objective
The aim of this work was to determine if it is possible to carry out EEG in children up to 4 years old without sedation and analyze the factors that could influence upon the possibility of performing EEG, in vigil or with sedation. Methods: In the period between November 2001 to November 2004, 489 patients up to 4 years old were studied in order to analyze how several parameters (sex, age, and diagnosis) could influence upon conditions of performing electroencephalogram (with or without sedation). Patients were assembled into several groups : sex, age (I: 0 – 12 months; II: 13 – 24 months; III: 25 – 36 months; and IV: 37 – 48 months), and diagnostic. The affections were : epilepsy, hyperkinesia, cerebral palsy, spasticity, sobbing spasm, encephalopathy, and psychomotor retardation.
Results
281 electroencephalographic studies were carried out in vigil and this value represented 57,5% of the total electroencephalograms performed. During the performance of the study the children’s behavior was independent of sex and initial diagnostic, but it was influenced by age. The higher number (104) of studied carried out in vigil was performed in children from 37 to 48 months, which represented 70,8 % of cases. The lowest percentage was obtained in children with psychomotor retardation
Conclusions
In most cases, it is possible to carry out electroencephalograms on children without using sedative drugs. To perform this study in vigil is advantageous because the recording of electroencephalographic signs in abnormal conditions of brain functioning and the appearance of contamination in the recording due to sedative drugs, which could confuse the diagnosis are avoided.
RESUME
Introduction
Bien que considéré comme inoffensive, la pratique de l’EEG sous sédation chez l’enfant n’est pas à l’abri de complications.
Objectif
Le but de l’étude est déterminer s’il était possible de pratiquer l’EEG chez l’enfant âgé 4 ans ou moins, sans sédation.
Méthodes
Entre novembre 2001 et novembre 2004, 489 patients âges de 4 ans ou moins ont été regroupés selon l’âge (groupe I: 0 – 12 mois ; groupe II : 13 – 24 mois ; groupe III : 25 – 36 mois; et groupe IV: 37 – 48 mois), le sexe, le diagnostic (épilepsie, hyperkinésie, paralysie cérébrale, spasticité, spasme en flexion, encéphalopathie, et retard psychomoteur au cours de la pratique de l’EEG, avec et sans sédation.
Résultats
281 EEG (57,5%) ont été réalisés chez des enfants en état de vigilance normale. Le comportement des enfants étaient indépendents du sexe et du diagnostic mais essentiellement influencé par l’âge. Les EEG ont pu être réalisés principalement chez les enfants (104) entre 37 et 48 mois (70,8 %). Le pourcentage le plus bas a été observé chez les enfants atteints d’un retard psychomoteur.
Conclusion
Il est possible de réaliser des EEG chez l’enfant sans sédation. De plus, une vigilance normale permet d’étudier l’activité électrique du cerveau sans artéfacts liés aux médicaments utilisés.
Keywords : Electroencéphalogramme, Enfants, Sédation, Technique, Electroencephalogram, children, sedation, Technic
INTRODUCTION
The term electroencephalogram (EEG) is used to refer to the electrical activity produced by the alive brain. This activity generated spontaneously can be monitored by electrodes. This approach produces no pain or uncomfort in patients (10).
Generally, electroencephalography is carried out in vigil, but nevertheless sedation is sometimes necessary to perform EEG on children. The use of sedative drugs is often associated with both the short age of the patient and the presence of an illness that hinders the correct study performing. Application of sedative drugs in EEG laboratories has several purposes:
a)it allows the application of electrodes without causing excessive anxiety
b)it permits recording with less muscle movements and
c)it allows recording of the asleep state (8).
Although it has been considered that sedation in children undergoing EEG tests is effective and safe and complications are infrequent (8), occasionally adverse sedation-related events are presented. This takes place especially with children having problems in the control of secretions (7); or when an overdoses or drug interaction is used (2). In addition, electroencephalographic recording with sedation is carried out in abnormal conditions of brain functioning, thus consequently some signals associated with the administration of sedative drugs are present and therefore, this situation could confuse the interpretation of the result.
It has been shown that it is possible to reduce the number of EEG studies with sedation (8). This strategy has some advantages, to perform EEG in a natural way, allows a better interpretation of results and the risks of sedation are avoided. In this way, parents and relatives are most satisfied.
In order to avoid the complications of sedative drugs, we carry out EEG in children up to 4 years old without sedation and analyze the factors that could influence upon the possibility of performing EEG, in vigil or with sedation.
MATERIALS AND METHODS
EEG study was carried out in 489 patients up to 4 years old, during the period from November 2001 until November 2004. When the use of sedative drugs was indispensable, children were sedated with barbiturate drugs by a specialized pediatrician in anesthesiology. When it was possible, EEG was performed without using sedative drugs. According with our work conditions, we developed a strategy to perform this study in vigil.
Patients studied were assembled into several groups as to sex, age (I: 0 – 12 months; II: 13 – 24 months; III: 25 – 36 months; and IV: 37 – 48 months), and diagnosis with which they arrived to the department. These affections were epilepsy, hyperkinesia, cerebral palsy, spastic lesion, sobbing spasm, encephalopathy, and psychomotor retardation. Finally, it was determined if the variables above mentioned had any influence upon the possibility of performing EEG in vigil or with the use of sedative drugs.
The statistical procedure was carried out using the professional software Statistic for Windows, Version 4.0, Copyright Statsoft, and Inc.1993. The study included the Kruskal-Wallis test. In such cases where this test was positive, a Mann-Whitney U test was conducted.
Methodology used to perform EEG in vigil
Preparation of the patient: Frequently children cry when they enter the EEG laboratory as response to the presence of unusual environment and unknown people. The first step is to reduce the child’s anxiety. With this aim, it is essential to establish communication between the nurse and the child. The interaction with these patients is carried out by means of a conversation. It should be explained, using a concrete terminology, the characteristics of the test and in children of short age, who do not understand the verbal language, it is necessary to use a corporal language in order for them to understand that EEG is not an aggressive study. The patient can thus interpret that this technique does not produce pain.
It is beneficial the parents’ presence during the study. They can help by offering their support and by demonstrating affection to the child. Previous to EEG study, parents should have received a complete explanation regarding the technique that will be applied to the child.
The room where EEG is going to be performed should have adequate conditions. Noises and interferences should be avoided. It is important that the technician requests to the doctor to limit the number of strange people that enters and leaves the laboratory during the procedure, because it could increase the patient’s anxiety.
Placement of electrodes: It is important to let the child use his/her favorite toys or others which would help in demonstrating the conducting of the study. It is recommended to have a group of toys in the laboratory, which can be used to explain the child how electrodes will be put in his/her head. In the cases in which children are not convinced with this method, it is recommended to give them the opportunity to put an electrode in the toy in order to diminish his/her fear.
The child is sustained in the bed or in the mother’s arms. The region in which the electrode is going to be placed is cleaned with alcohol and a cleaner substance in order to reduce the impedance electrode-skin. Later, a conductive gel is applied which, at the same time, is adhesive and it holds the electrodes. Disk scalp electrodes that are placed according to the 10-20 International System are used (6). The impedance electrode-skin should be verified and it should not be higher than 20 kW.
Electroencephalographic recording: During the performance of EEG study it is useful that parents sing children’s songs or relate children’s stories to the child, by using a very soft tone of voice. Consequently, the children will be distracted and the performance of the study will be easier.
During the study some maneuvers are carried out such as to close and open the eyes, hyperventilation, and photo stimulation. The performing of these maneuvers is achieved, when the nurse imitates the behavior that is requested from the child. The parents’ collaboration for carrying out all these maneuvers is important. To carry out hyperventilation, one should request the child to do like when he blows the candles of his/her birthday cake or when he/she inflates a balloon. To carry out the photo stimulation, it is explained to the child that the approach is like to take some birthday pictures. In general, working with the children’s imagination can be possible to obtain better results.
RESULTS
The methodology used in our department, in order to perform EEG in vigil, was adequate. The number of EEGs carried out with the use of sedative drugs in children of short age was thus reduced.
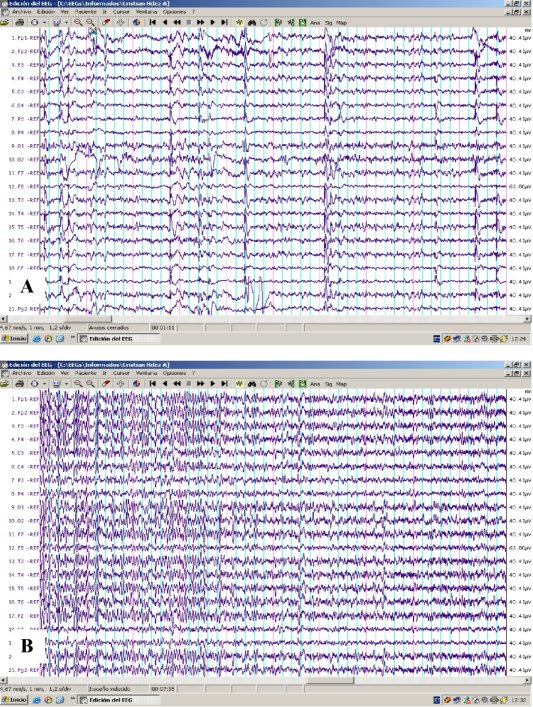
The quality of EEGs recording performed in vigil was higher due the contamination of the recording was avoided. Figure 1 shows the difference in the quality of the EEG recording, carried out in the same child, first without sedation and later using sedative drugs.
From a total of 489 children studied by electroencephalography, 208 studies were carried out using sedative drugs and 281 of them were studied in vigil. Thus, 57,5% of the total studies did not need the application of sedation. 100 % of the EEGs performed in vigil were successful.
From the 281 EEG performed without application of sedative drugs, 126 were girls (44,8 %) and 155 were boys (55,2 %). In spite of the differences between the number of boys and girls studied in vigil, significant differences were not found between both groups.
Forty-three EEG in vigil were performed in children up to one year old, this value represented 52,4 % of studies carried out without the use of sedative drugs. Sixty-four studies in vigil (47,4 %) were performed in children that belonged to the 13 – 24 months group. Seventy children from 25 to 36 months (56,0 %) were studied by EEG without sedation.
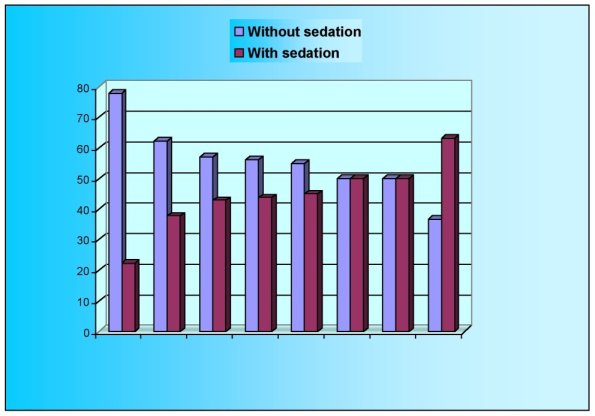
The higher number (104) of studied carried out in vigil was performed in children from 37 to 48 months, which represented 70,8 % of cases (figure 2). The number of children from groups I and II performed in vigil were significantly different to the number of studies carried out in the same conditions belonging to group IV (p<0.001). As it was expected this behavior was the same for the group of children studied in sedation.
Figure 2 shows the percentage of electroencephalographic studies performed both in vigil and with sedative drugs regarding the different diagnosis with which patients arrived to the EEG laboratory. For all affections, the percentage of EEG carried out without the use of sedation was equal or higher than 50 %, except for Psychomotor Retardation. The highest percentage of EEGs carried out in vigil, in descendent order, was obtained in children with hypyperkinesia, epilepsy, spasticity and cerebral palsy. The lowest percentage was obtained in children with psychomotor retardation. Although there were no significant differences among the number of studies performed in vigil, as to the different diagnosis, the number of EEG performed without sedation had a clear tendency to increase in children with the diagnosis of hyperkinesia and Epilepsy. Whereas in children with diagnosis of psychomotor retardation, there was a tendency to decrease.
DISCUSSION
It is well known that the use of sedative drugs is always accompanied of several risks. Cote et al. demonstrated that a high percentage of children suffer drug-related adverse outcomes after administration of a wide variety of medications (1). They observed that negative outcomes were associated with all classes of drugs and ways of administration (2, 3). In spite of these risks observed in children, associated to sedation, it has been exposed that sedation in children during the EEG procedure is effective and safe and complications are infrequent (8). Nevertheless, we considered that in our conditions of work, it could be possible to develop a methodology for carrying out the electroencephalography in children without using sedative drugs. EEG is a study that does not cause pain, consequently it was conceivable to perform the examination in a great percentage of children avoiding the utilization of sedative drugs.
As far as we are concerned, the development of a methodology to perform the EEG in vigil was advantageous. The parents and/or relative accompanying children who underwent the study in vigil were more satisfied. Also, the quality of EEG recording in the cases in which sedation was not used was better because the appearance of typical signals due to sedative drugs were avoided (Figure 1). The muscle movements that are reflected in the recording when sedation is not used did not hinder, in any case, the interpretation of the result. This outcome can be explained due to the patient’s anxiety was decreased by means of the interaction with the technician. For this reason, the interpretation of the result by the specialist was easier and safer.
A total of 281 studies (57,5 %) were performed without application of sedative drugs. These results are similar to those obtained by Olson et al. (8). They were able to decrease the proportion of children requiring sedation from 32 % to 2 %, using behavioral techniques to decrease the child’s fear. There have been several opinions regarding the study of Olson et al. (1,5). Nevertheless, by all means, these researchers have developed an adequate strategy to perform EEG in vigil on children.
From the EEGs carried out in vigil, 44,8 % were girls and 55,2 % were boys. Our results indicate that sex did not influence on the patient’s behavior regarding the possibility to perform the EEG in vigil or under sedation. Although generally girls are more docile than boys, if children would be able to understand that the study is not an invasive approach and they do not perceive fear, it will be easy to carry out EEG in vigil.
As it is shown in figure 2, the age of children influenced on the behavior of performing EEG in vigil. Higher difficulties to carry out the electroencephalographic study in vigil are presented in children of up to 2 years of age. With an increase of the children’s age, there is a decrease in the need to use sedative drugs. This behavior could be justified because children of more age understand better the explanation given by the technician. Thus, in these cases, for the technician is easier performing the study without sedation.
Higher difficulties for performing the EEG in vigil were presented in children with diagnosis of Psychomotor Retardation. These results were influenced by characteristics of patients with this affection. In these patients there is retardment in the learning process and in social abilities, which makes the technician-child interaction more difficult (4).
It was relatively easier to carry out the study without sedative drugs, in children with diagnosis of epilepsy and hyperkinesia. The pathophysiology of these affections, which is associated with neurochemistry disturbances (9) do not hinder, in most cases, that children establish social interaction allowing them to understand the technician explanation.
We consider that although it is more difficult to perform EEG in vigil on children of less than 4 years, in most cases, it is possible to increase the number of studies carried out in vigil by reaching a better interaction between technician and patients.
CONCLUSION
The results of this study demonstrated that, in most cases, it is possible to carry out electroencephalograms on children without using sedative drugs.
TABLE 1: Number of EEGs performed in vigil and with sedation for each group of age.
| Group of ages |
EEGs performed with sedation |
EEGs performed in vigil |
Total of EEGs performed |
| I |
39 (47.6 %) |
43 (52,4 %) |
82 |
| II |
71 (52,6 %) |
64 (47,4 %) |
135 |
| III |
55 (44,0 %) |
70 (56,0 %) |
125 |
| IV |
43 (29,2 %) |
104 (70,8 %) |
147 |
REFERENCES
- COTÉ CJ. Sedation for Electroencephalogram. Pediatrics 2001;108:1053-1054.
- COTÉ CJ, KARL HW, NOTTERMAN DA, WEINBERG JA, McCLOSKEY C. Adverse Sedation Events in Pediatrics: Analysis of Medications Used for Sedation. Pediatrics 2000;106:633-644.
- COTÉ CJ, NOTTERMAN DA, KARL HW, WEINBERG JA, McCLOSKEY C. Adverse Sedation Events in Pediatrics: A critical Incident Analyisis of Contributing Factors. Pediatrics 2000;105:805-814.
- FERNÁNDEZ E. Desarrollo Psicomotor. In FEJERMAN N, FERNÁNDEZ E eds. Neurología Pediátrica 1997. Buenos Aires: Panamericana p 24-33.
- FREEMAN JM. The Risks of Sedation for Electroencephalograms: Data at Last. Pediatrics 2001;108:178.
- JASPERT HH. The Ten Twenty Electrode System of the International Federation. Electroenceph Clín Neurophysiol 1958;10:371-375.
- NAPOLI K, INGALL C, MARTIN G. Safety and efficacy of chloral hydrate sedation in children undergoing echocardiography. J Pediatric 1996;129:287-291.
- OLSON D, SHEEHAN M, THOMPSON W, HALL P, HAHN J. Sedation of Children for Electroencephalograms. Pediatrics 2001;108:163-165.
- QUIÑONEZ-NÚÑEZ M., LIRA-MAMANI D. Perfil epidemiológico de la epilepsia en una población hospitalaria en Lima, Perú. Rev Neurol 2004;38: 712 – 715.
- SÁNCHEZ A, PADILLA E, ZALDIVAR M, MORALES L. Electroencefalograma digitalizado. Metas de Enfermería 2003;VI:20-24.
