
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ORIGINAL PAPERS / ARTICLES ORIGINAUX
A COMPARISON OF STROKE KNOWLEDGE BEFORE AND AFTER EDUCATION IN ETHIOPIA (THE ASK PROJECT)
CONNAISSANCES SUR LES ACCIDENTS VASULAIRES CEREBRAUX AVANT ET APRES UNE EDUCATION EN ÉTHIOPIE (PROJET ASK)
E-Mail Contact - ZEWDU Ruth :
Sonja.Stutzman@UTSouthwestern.edu
ABSTRACT: Background: In order to address the growing burden of stroke in Africa, it is essential to have teaching tools that are accessible to a wide variety of communities. Resources for stroke, recognition of symptoms, steps to assist a stroke victim, or any educational tools are scarce. In order to increase education about stroke, we introduced a stroke education intervention in Bahir Dar, Ethiopia in the Amharic language. The aim of the intervention was to see if stroke knowledge and recognition of stroke symptoms increased post-education. Methods: An anonymous pre-test questionnaire was given to identify their baseline stroke knowledge, and then participants viewed the video about stroke. The Amharic BE-FAST acronym was introduced in the video to evaluate participants’ retention of stroke symptoms, while emphasizing the importance of rapid response. Participants were given a survey to post-test survey of their short-term memory recall, along with another satisfaction survey. Results: Over 50% of participants remembered all five letters of the Amharic BE-FAST acronym, nearly 80% answered that they learned about stroke prevention, 90% were satisfied with the video, and 98% thought it should be available widely to the general public. The data presented showed that there was an improvement in stroke education retention with the use of the stroke education video. Conclusions: The Amharic BE-FAST acronym demonstrated to be an effective tool in communicating the symptoms of stroke from English to Amharic. Stroke education was well received, which provided insight on how to design and implement new medical concepts in native languages. Keywords: Amharic stroke acronym, education, global health, neurology education, stroke. RESUME Introduction: Afin de faire face au fardeau croissant des AVC en Afrique, il est essentiel de disposer d’outils pédagogiques accssibles à une grande variété de communautés. Les ressources pour l’AVC, la reconnaissance des symptômes, les étapes pour aider une victime d’AVC ou tout autre outil éducatif sont rares. Afin d’accroître l’éducation sur l’AVC, nous avons introduit une intervention d’éducation sur l’AVC à Bahir Dar, en Ethiopie, en langue amharique. Le but de l’intervention était de voir si la connaissance et la reconnaissance des symptômes de l’AVC augmentaient après l’éducation. Méthodes: Un questionnaire pré-test anonyme a été donné pour identifier leurs connaissances de base sur l’AVC, puis les participants ont visionné la vidéo sur l’AVC. L’acronyme amharique BE-FAST a été introduit dans la vidéo pour évaluer la rétention des symptômes d’AVC par les participants, tout en soulignant l’importance d’une réponse rapide. Les participants ont reçu une enquête pour post-test de leur mémoire à court terme, ainsi qu’une autre enquête de satisfaction. Résultats: Plus de 50% des participants se sont souvenus des cinq lettres de l’acronyme amharique BE-FAST, près de 80% ont répondu avoir appris la prévention des AVC, 90% étaient satisfaits de la vidéo et 98% pensaient qu’elle devrait être largement accessible au grand public. Les données présentées ont montré qu’il y avait une amélioration de la rétention de l’éducation sur l’AVC grâce à l’utilisation de la vidéo d’éducation sur l’AVC. Conclusion: L’acronyme amharique BE-FAST s’est révélé être un outil efficace pour communiquer les symptômes de l’AVC de l’anglais à l’amharique. L’éducation sur l’AVC a été bien accueillie, ce qui a permis de comprendre comment concevoir et mettre en œuvre de nouveaux concepts médicaux dans les langues maternelles. Mots-clés : Acronyme amharique de l’AVC, AVC, Education, Education en neurologie, Santé mondiale.
INTRODUCTION Each year, 15 million people suffer from stroke worldwide (4). Nearly 80% of strokes are associated with preventable risk factors, and efforts in the United States (US) have been devoted to stroke education and determination of the risk factors, as well as the importance of time from symptom onset to treatment. Yet, stroke is a global issue that impacts people around the world and there is little attention given to stroke due to multiple complexities. Language and understanding of the disease are a common barrier in low to middle-income countries. For example, the Amharic language currently does not have a widely recognized medical term for “stroke”. The purpose of this project is to introduce an education module in Bahir Dar, Ethiopia about stroke in the Amharic language, and assess stroke knowledge before and after the education. This education module has been previously used to educate Amharic speaking immigrants in the US and there is now an opportunity to expand this education to Ethiopia. BACKGROUND An ischemic stroke occurs when an interruption in blood flow to an area of the brain deprives the cells of oxygen, causing the cells to die. Because stroke is a major cause of mortality and disability in America, the American Heart Association seeks to prevent the causes of strokes in various populations. This effort has decreased the stroke incidence over the years. However, in certain races and populations, mortality and morbidity from stroke remains high. In the US, seven million Americans over the age of 20 reported having a stroke in 2016 (6). In 1990, the stroke burden was approximately 38 million disability adjusted life years and this is projected to rise to 61 million disability adjusted life years by 2020 (4). Until recently, there was very little research on the prevalence, rate of disability, mortality and morbidity rates, and risk factors in Africa. For example, the work done by Mayowa O Owolabi and his team in Cardiovascular Journal of Africa attempted to examine these elements in Africa, but with few resources on the patterns of stroke outcome and burden the conclusion was indeterminate. Additionally, there is still no research available specifically on the impact of stroke education in Africa (10). The lack of education and awareness on disease in lower income countries has led to a growing global burden when it comes to stroke. Globalization has proven to be a vital determinant in the prevention of chronic non-communicable diseases (9). The US has focused on catchy phrases such as, Time is Brain and BE-FAST to assist people in understanding stroke and ways to intervene when a stroke is occurring. The Time is Brain Campaign involves the importance of time when symptoms of a stroke occur and also in treating stroke patients. The longer therapy is delayed, due to not calling an ambulance or going to the hospital, the lesser the chance it will be successful. The BE-FAST campaign involves using the acronym to learn the signs and symptoms of stroke and to act quickly when the symptoms are recognized. The dissemination of knowledge and information from countries, such as the US, to other nations aids in the awareness of the populations in those countries on stroke (8). Studies have shown that education tools and programs that are started within the community lead to increased awareness of strokes and shorten the time of presentation at the hospital, making them better candidates for intervention (6). However, other studies such as Racial/ethnic disparities in mortality by stroke subtype in the United States have also revealed that the people at a socioeconomic disadvantage tend to have poorer results and relations with healthcare communities, which might factor into their increased mortality rates from strokes (3). A more recent body of literature supports that increasing stroke awareness has led to positive health outcomes for individuals at risk (7). The spread of knowledge and information about stroke awareness has the potential to help in the prevention and management of this disease. In order for these populations to be knowledgeable of stroke prevention and how to manage these situations, it would be beneficial if stroke education is given in the native language of the recipient, so that it may be fully understood in a language that is understandable and culturally acceptable for the population in need. The aims of this study are to assess participant stroke knowledge, recognition of stroke signs, risk factors and symptoms before and after watching the stroke education video in Amharic. METHODS This stroke education research project is a part of the larger Bahir Dar Outreach for Neurology Education (BORNE) initiative, which involves building institutional capacity of the region by collaborating in neuroscience education and research. The study was a prospective pre/post-test cross-sectional design, which took place in Bahir Dar, Ethiopia. Prior to recruitment, an educational video was developed by the Principal Investigator (PI) and the research team. The video introduces signs and symptoms of a stroke, ways to prevent stroke, and the BE-FAST acronym. All of the data presented in the video was based on the American Heart Association Guidelines and was presented in the Amharic language by the PI, an American physician from Ethiopia. Participants were recruited from hotels, restaurants, markets and clinics to survey a diverse population. Participants completed a demographic survey (age, education, children in household, marital status) and an anonymous pre-test questionnaire in Amharic to identify the baseline level of knowledge of stroke signs, symptoms, and risk factors, followed by a short (approximately 5 minutes) video presentation, which included the Amharic version of the BE-FAST acronym. After watching the video, participants were given a post-test survey in Amharic to measure short term memory recall (Table 1). Additionally, a satisfaction survey in Amharic was administered to determine how well participants liked the stroke education video (Table 2). Survey data was collected for two weeks. All surveys were anonymous. The study was approved by the local Institutional Review Board in the US prior to data collection. RESULTS Of the 118 participants enrolled in the study (Table 1), 3 participants were under the age of 18, 104 were between 18 to 44 years of age and 10 were between 45 to 64. Sixty-eight of the participants were male (58%). The average household contained 4.5 individuals. The majority of participants were single (65%) or married (32%). Tertiary or university education was the most common form of education (66%), followed by secondary education (21%). Amharic was the primary language spoken by 116 of the 118 participants. Approximately three-quarters (74%) of participants correctly identified all the symptoms as common signs of stroke during the pre-test section. In regard to stoke knowledge (Table 2), more than half (63%) of the participants identified that stroke is not another name for “heart attack”. Approximately, 75% of participants thought that diabetes could cause a stroke and 44% thought that drinking 3-4 beers daily could cause a stroke. Seventy-seven percent of participants answered that blood pressure management is the most important way to prevent a stroke. If participants thought they were having a stroke, 80% reported they would call a family member or friend to drive them to the doctor, and 94% of participants stated if they think they are having a stroke, they will seek medical attention. After watching the educational video, participants were asked to remember the acronym for signs and symptoms of a stroke that was translated from the BE-FAST acronym. The acronym was translated from English to Amharic in the video and in the post-test survey (Figure 1). Of the 118 participants, 62 could remember all 5 letters of the acronym, 14 could remember 4 of 5, 10 could remember 3 of 5,11 could remember 2 of 5, 7 could remember 1 of 5, and 11 participants could not remember any of the 5 letters of the acronym. The participants were also asked to complete a satisfaction survey following the completion of the video (Table 3). The satisfactory survey showed 80% of the participant responded positively and reported that they learned more about stroke prevention. Of the participants, 91 % were satisfied with the video they saw and 98% thought that this teaching should be available for the public. DISCUSSION The participants in this study reported that they were generally satisfied with the education they received. Additionally, the majority of the participants were able to recall over half of the BE-FAST acronym presented in the video. The combined satisfaction and education recall made the research study a success. The participants in the study reported a positive experience and that they were likely to share this information with others. This information alone has the potential to impact the Bahir Dar community in a positive way, as previous studies have shown that community based learning can have positive outcomes (5). The demographics of this study are reflective of young educated persons living in a metropolitan area of Ethiopia. This may be due to the recruitment locations in downtown Bahir Dar, Ethiopia were prime locations for young adults to socialize and included: restaurants, coffee shops, malls, and soccer fields. This follows the trajectory of other research completed in the US that shows that those of a higher socioeconomic status have greater access to education and prevention (1, 2). The researchers experienced that many of the women felt shy, inadequate, and uncomfortable to participate in the survey, resulting in a greater percentage of male participants. Understanding the research population allows for further understanding of the predicted stroke knowledge gap. The researchers had a time limit and a limited experience with the Ethiopian culture prior to this trip. Future research with the Amharic speaking community may benefit from recruitment of a more diverse sample. The education video achieved the goal of providing adequate education at a level that was appropriate for the recruited population. The research team was careful to present culturally sensitive information that also followed the American Heart Association Guidelines. By featuring a native Ethiopian speaker, who is also a stroke expert in the US, the video was both educational and appropriate for this population. Participants correctly responded to 89% of the stroke knowledge true/false questions. There were 90% of participants who recognized that if they believed they were having a stroke; they should seek immediate medical attention. Being able to recognize a medical emergency is the first major step towards a better outcome. In the “recognition of acronym” section, the “BE-FAST” acronym was translated into the Amharic as “እሚፈጥን” pronounced “eh-mi-fe-ti-n”. This section of the post-test took longer to complete, yet over 50% of participants answered all 5 of the “BE-FAST” acronym questions correctly (Figure 1). These results show the efficacy of the stroke intervention education presented in the language of the target population, in increasing knowledge of stroke symptoms. In the satisfactory survey responses, participants shared their feedback on the overall experiment. Their commentary and feedback regarded their confidence in stroke education, satisfaction on the video, and the suggestions on how to improve the research. Over 85% of participants had exceptionally positive responses to the study. There were 86% who strongly agreed that stroke education should be available to the public. Overall, when introducing a new medical concept, it is helpful to provide brief, accessible, culturally sensitive information in their native language. Introducing a new concept in a language and culture that is different from that of the US has its challenges, but the post-test and satisfaction scores of this study show that it can be done successfully in a short amount of time using the community based education models that have shown success in the US. Limitations Some limitations of the study stemmed from difficulties with communication. Some participants filled out the form while the video was being shown instead of after, which may not have accurately depicted their view on the video’s actual educational value or what information they retained. Part of the problem was the video may have been too long and participants may not have wanted to or been able to watch the full presentation. At times, participants complete the study in small groups, which could limit our understanding of how well each of them actually understood the material on their own. Some participants also were not able to complete the survey in its entirety. The study sample may not be representative of all regions in Ethiopia as a whole. Further research can give participants in a wider array of age groups and increase the validity between correct and incorrect responses on the evaluations. CONCLUSION This stroke education research project is a part of the larger Bahir Dar Outreach for Neurology Education (BORNE) initiative, which the PI is pursuing. These types of global outreach initiatives have a potential to grow stroke education research in countries like Ethiopia. The lessons learned from the ASK project will provide a better understanding of how to design stroke education tools for the larger Ethiopian population going forward. The satisfaction with the material presented was significant and there is a desire to make it widely available. The study showed that a brief educational video, that is accessible in the participant’s language with culturally sensitive material, can assist in retaining new information about what a stroke is and what steps to take when symptoms of a stroke occur and what steps to take to prevent stroke in the first place.
Tables and Figures Table 1: Descriptive Statistics
Table 2: Stroke Knowledge Questions (Pre-Test)
Table 3: Satisfaction Survey Responses (Post-test)
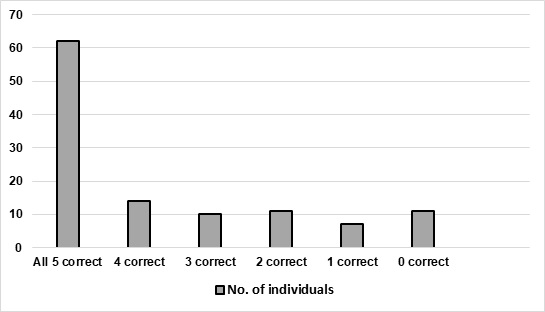 Figure 1: BE-FAST Acronym Translated from English to Amharic answered correctly REFERENCES
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
© 2002-2018 African Journal of Neurological Sciences.
All rights reserved. Terms of use.
Tous droits réservés. Termes d'Utilisation.
ISSN: 1992-2647