
|
|||||||||
|
CLINICAL STUDIES / ETUDES CLINIQUES
NORMATIVE VALUES OF THE BLINK REFLEX
VALEURS NORMATIVES DU REFLEXE DE CLIGNEMENT
E-Mail Contact - ABOUBACAR NAHANTCHI Abdourahaman :
anainterne@yahoo.fr
SUMMARY Background The blink reflex (Blink Reflex) is a non-invasive electrophysiological exploration technique. It allows to study the proximal conduction of the facial and trigeminal nerves. In addition, it also allows to explore the brainstem. Objective The objective of our study was to establish the normative values of the blink reflex at the neurophysiology laboratory of the Fann National University Hospital Center in Dakar-Senegal. Methodology The study population consisted of 30 healthy adult subjects who volunteered to participate in the study, ranging in age from 18 to 59 years old. This was a cross-sectional study, over a period of two months, from March 1st to April 30th, 2019.The electromyography machine used was a Medelec Synergy (OXFORD) device. The recording of the blink reflex allowed to obtain an early R1i (ipsilateral) response and two late responses, R2i and R2c which was contralateral. Results The mean latency of the R1 response was 10.7 +4 ms with extremes between 9.9 ms and 11.8 ms. The mean latency of the R2 response was 33.3 ±3.3 ms with a minimum at 26 ms and a maximum of 40 ms. The mean response latency R2c (contralateral) was 33.5 ±3.6 ms with a minimum of 27 ms and a maximum of 41 ms. Conclusion Our work shows average latencies: R1 at 10.7ms, R2 at 33.3ms and R2c at 33.5ms. Keywords: Blink reflex, normative values, Senegal RESUME Introduction Le réflexe de clignement (Blink Reflex) est une technique d’exploration électrophysiologique non invasive. Il permet d’étudier la conduction proximale des nerfs faciaux et trijumeaux. En plus il permet aussi d’explorer le tronc cérébral. Objectif L’objectif de notre étude était d’établir les valeurs normatives du réflexe de clignement du laboratoire de neurophysiologie du centre hospitalier national universitaire de Fann Dakar-Sénégal. Méthode La population d’étude était composée de 30 sujets adultes sains se portant volontaires pour participer à l’étude, avec un âge compris entre 18-59 ans. Il s’agit d’une étude transversale, sur une période de deux mois, allant de 1er mars au 30 avril 2019.L’appareil d’électromyographie utilisé était un appareil Medelec Synergy (OXFORD). L’enregistrement du réflexe de clignement a permis d’obtenir une réponse précoce R1i (ipsilatéral) et deux réponses tardives R2i et R2c controlatérale. Résultats La latence moyenne de la réponse R1 était de 10,7 +4 ms avec des extrêmes à 9,9 ms et 11,8 ms. La latence moyenne de la réponse R2 était de 33,3 ±3.3 ms avec un minimum à 26 ms et un maximum à 40 ms. La latence moyenne de la réponse R2c (controlatérale) était de 33,5 ± 3,6 ms avec un minimum à 27 ms et un maximum à 41 ms. Conclusion Il ressort de notre travail des latences moyennes : R1 à 10,7ms, R2 à 33,3 ms et R2c à 33,5ms. Mots clés : Blink reflexe, normes, Sénégal INTRODUCTION The blink reflex is a non-invasive electrophysiological exploration technique. It is a polysynaptic reflex, physiologically organized as a flexion reflex (6). It allows to study the proximal conduction of the facial and trigeminal nerves (5). This reflex also makes it possible to explore the brainstem. It is composed of two sides. The facial nerve is the efferent side and the afferent side is provided by the trigeminal nerve (V) (5). Recording the blink reflex results in a response R1 and R2 ipsilateral to the stimulation and a response R2 Contralateral to the stimulation (5). Indeed, each laboratory must establish these standards. For this purpose, we carried out a study at the neurophysiology laboratory of the Fann National University Hospital Center (CHNU) whose objective was to establish the normative values of reflex blinking. MATERIALS AND METHODS Our study was conducted at the Clinical Neurophysiology Laboratory of The Neurosciences Department Pierre Ibrahima Ndiaye, CNHU FANN, Dakar, Senegal. This was a cross-sectional and descriptive study, over a period of two months, from March 1st to April 30th, 2019. The study included all healthy adult subjects practicing at the Ibrahima Pierre Ndiaye Neuroscience Department, CNHU of FANN, Dakar -Senegal aged from 18 to 59 years old, volunteering to participate in the study. The electromyography device used was a fixed (OXFORD) device (Figure 1); it was connected by a stimulator that generates electrical currents allowing transcutaneous stimulation in a single or repetitive mode. The electrode used for stimulation is a bipolar electrode (Figure 2). The electrodes used for the collection were self-adhesive patch electrodes (Figure 3). They were connected to an amplifier allowing multichannel recordings (channel 1, 2). After explaining the examination, the volunteer was placed in a semi-recumbent position on the examination bed. He was asked to relax, without clenching his teeth, and to turn off his phone to avoid interference. The room was maintained at an optimum room temperature (22-27°C). The first step was to use ether strip the skin the orbicularis muscle of the eyelids and the skin of the forehead. Then the second step was to place the collection electrodes, active in the middle of the lower orbital edge just below the lower eyelid. The collection electrodes were placed left and right as follows: The active electrode on the eyelid orbicularis in the middle of the lower orbital edge, just below the lower eyelid and the reference, 2 cm laterally. For stimulation, the cathode was placed on the supraorbital notch, at the internal 1/3 middle-1/3 union of the superior orbital rim, the anode was placed 2-3 cm higher and turned outside with an oblique angle, to avoid the diffusion of the current to the contralateral sus-orbital nerve (Figure 4). The stimulation intensity used was between 15 to 25 mA. In our study, an intensity of 25 mA was used, resulting in almost stable reflex responses of maximal amplitude, with a stimulation duration of 0.1ms. The supraorbital nerve on both sides (right and left) was stimulated successively and the subject keepeds his eyes open. Three responses were recorded: an early ipsilateral R1 response and two late responses: ipsilateral R2 and contralateral R2 (Figure 5). Data was collected from the report in the ENMG (OXFORD). The variables studied were socio-demographic characteristics (age, sex, weight, height, place of residence), the mean latencies of the responses (the early ipsilateral R1i response, the late ipsilateral R2i responses and the R2c Contralateral) and the difference latency response between the right and left side. The data capture and processing were carried out with the software Microsoft world 2013, Epi info in its version 3.5.1 and Microsoft Excel 2013. We calculated frequencies, means of the early responses (R1i) and late responses (R2i and R2c) with standard deviations. RESULTS From a total of 32 healthy adult volunteers, 30 were included in the study. The mean age of volunteers was 33.7 years with a minimum of 20 years and maximum of 57 years. Men accounted for 63.3% and women accounted for 36.7%, with a sex ratio of 1.7. The mean height of volunteer was 1.72 m with a minimum of 1.50 m and a maximum of 1.87 m. The mean weight of the subjects was 68 kg with a minimum of 30 kg and a maximum of 90 kg. All volunteers resided in the city of Dakar. Regarding the average latency recorded, the R1 response was 10.7 ±4 ms with extremes from 9.9 ms to 11.8 ms. The R2 response was 33.3 ± 3.3 ms with a minimum of 26 ms and a maximum of 40 ms. The response R2c (contralateral) was 33.5 ±3.6 ms with a minimum of 27 ms and a maximum of 41 ms (Table I). Depending on the side (right or left) studied responses (early and late) were recorded. Thus, for the right side, the average latency of the R1i (ipsilateral) response was 10.7 ms with a minimum of 9.9 ms and a maximum of 11.8 ms, that of R2i (ipsilateral) was 33.4 ms with a minimum of 27.7 ms and a maximum of 40 ms. Finally, the average latency of the response R2c (contralateral) was 33.5 ms with a minimum of 28 ms and a maximum of 41 ms (table). For the left side, the average latency of the R1i (ipsilateral) response was 11 ms with a minimum of 9.9 ms and a maximum of 12 ms, that of R2i (ipsilateral) was 33.2 ms with a minimum of 26 ms and a maximum of 41 ms. The average response latency R2c (contralateral) was 33.4 ms with a minimum of 27 ms and a maximum of 40 ms. The difference between the averages of the R1 responses between the two sides (right-left) was 0.3 ms (p = 0.7946), that of R2 was 0.2 ms (p = 0.8954) and for R2c it was at 0.1 ms (p = 0.9954). DISCUSSION The mean age of the subjects was 32.8 years with a minimum of 20 years and a maximum of 57 years. In our study the subjects were young, and the male sex was the majority (63.3%). Medvedeva had conducted a similar study to ours in healthy young subjects (7). The height of the subjects in our study ranged from 1.50 m to 1.90 m. Brooks (2) reported in his study heights between 1.50 m and 1.90 m similar to those observed in our work. The average latency of the R1 response observed in our study was 10.7ms. In France, Fournier reported an interval of 10-11ms as expected values for the R1 response. Brooks in Brazil reported on a series of 400 volunteers, a latency R1 at 10.30ms (2), the latter is slightly lower than that obtained in our work. Mora-Brambila, in Mexico, in a series of 20 healthy subjects, an average latency of R1 (11 ms) was higher than that obtained in our study (8). In addition, Denen in his cohort also obtained R1 latency (11 ms) greater than that of our study (3). On the other hand, Pierre Guihéneuc in France had reported a mean latency R1 (10.1 ms) lower than that obtained in our study (8). In Korea, BAE (1) reported a mean latency of the R1 response lower than that obtained in our study. There was a variation in the mean value of R1 latency according to the studies. This variation was also found by Brooks, and Medvedeva (2,7). The reasons of this variation were multiple. It might be a difference in the technique. As an example, some authors have used for the recording small concentric needle electrodes with the advantage of eliminating the contamination of the responses of the eyelid orbicularis by those of the masseter muscle. Thus, Pierre Guihéneuc (6) used small needles for the reception which allowed him to record the weak latencies, unlike our study where patch electrodes were used, resulting in a slightly higher latency than Pierre Guihéneuc. In our work, the average latency of the R2 response was 33.3 ms. The average latency of the R2c response (contralateral) was 33.5 ms. Medevedeva reported in his cohort of 31 healthy subjects slightly similar results to ours with an average latency of R2 at 33.1 ms and R2c at 34.3 ms. The similarity of the R2 and R2c latency values of our study to that of Medevedeva was explained by the fact that the size of the studied population and the technique (collection and stimulation) used in the Medevadeva study was approximately identical to our work (7). Stimulation of the left supraorbital nerve in our study resulted in contralateral R1 (ipsilateral), R2 (ipsilateral), and (R2c) responses with mean latencies of 11 ms, 33.2 ms, and 33.4 ms respectively. Compared to our results, lower latencies were observed in the BEA (1) study. However, the average R1 latency obtained in our study was similar to that reported by Mora-Brambila but the latency R2, R2c of the latter was lower than ours (8). Table II, illustrates the comparison of the response of R1, R2, and R2 controlateral of our study with that of the different authors.Stimulation of the right sus-orbital nerve in the BEA study yielded the responses R1 (ipsilateral), R2 (ipsilateral) and R2c (contralateral) with mean latencies R1 at 9.58 ms, R2 at 26,69 ms and R2c at 27.32 ms (1). In opposite, our results are superior to those reported by Brooks (2). However, Mora-Brambila reported R1 latency similar to ours but the R2, R2c responses were lower than those of our study (8). The difference in average latencies between the sides was 0.3 ms for R1, 0.2 ms for R2 and 1.4 ms for R2c. This difference between the two sides was not statistically significant. A difference in latency R1 (0.42 ms) similar to that of our work was found in the study, but the difference in latency R2 (1.9 ms,) was higher than ours (1). Preston reported a difference in R2c latency of less than 7 ms. the latter is greater than that obtained in our study (9). CONCLUSION The blink reflex is a mean of electrophysiological exploration to explore the proximal segment of the trigeminal and facial nerves. In addition, it also allows to explore the brainstem. In order to interpret the result of this reflex, normal values must be known and established for each electrophysiology laboratory. Our work shows average latencies: R1 at (10.7ms), R2 at (33.3ms) and R2c at (33.5ms). This is a preliminary study with a small population size. Indeed, it would be necessary later to establish a cohort large enough to have statistically representative data.
 Figure 1: Electromyography device Medelec Synergy (Oxford)
 Figure 2: Bipolar electrode of stimulation
 Figure 3: Self-adhesive patch electrodes
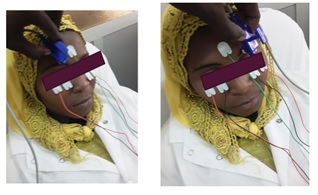 Figure 4: Blink Reflex stimulation
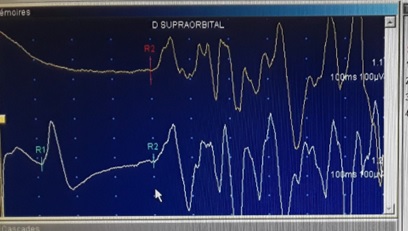 Figure 5: Normal responses R1i, R2i and R2c
Table I: Distribution of average latencies of responses
Table II: Comparison of averages of latencies responses
Conflicts of interest All the authors do not have any possible conflicts of interest REFERENCES
conduction alterations in leprosy patients. LeprRev. 2006 Jun;77(2):114-20.
|
© 2002-2018 African Journal of Neurological Sciences.
All rights reserved. Terms of use.
Tous droits réservés. Termes d'Utilisation.
ISSN: 1992-2647