
|
|
|
ORIGINAL PAPERS / ARTICLES ORIGINAUX
VALIDATION OF THE SIX ITEM COGNITIVE IMPAIRMENT TEST (6CIT) AS A SCREENING TOOL FOR COGNITIVE DYSFUNCTION IN PATIENTS WITH PARKINSON’S DISEASE
Validation du test d’altération cognitive à six éléments (6CIT) en tant qu’outil de dépistage du dysfonctionnement cognitif chez les patients atteints de la maladie de Parkinson
Abstract Background Parkinson’s disease (PD) is a chronic neurodegenerative disorder associated with cognitive dysfunction resulting in increased caregiver burden, pressure on community health facilities and mortality in affected patients. There is paucity of data from Sub-Saharan Africa as most of the data concerning cognitive dysfunction in PD are from studies done in Europe and North America. Objective This study aimed to validate the Six item Cognitive Impairment test (6CIT) as a screening tool for cognitive dysfunction in patients with PD and to determine the frequency , pattern and predictors of cognitive dysfunction in these patients. MATERIALS AND METHODS This was a cross sectional case control study carried out at a tertiary health facility in South-south Nigeria. Cognitive performance of thirty patients with PD were compared with thirty demographically matched controls using two neuropsychological test batteries namely, the Iron psychology (FePsy) and the Six item Cognitive Impairment (6CIT) tests. Results The frequency of cognitive impairment using the 6CIT in patients with PD was 53% (3.3% for controls). The cognitive domains studied encompassed memory, language, executive dysfunction, psychomotor speed, and constructional apraxia. The patients with PD performed poorly in all cognitive domains of FePsy with significant p values except the binary choice reaction time (p=0.051) and non-dominant hand on finger tapping (p=0.138). The independent predictors of the overall cognitive impairment in the patients with PD using logistic regression analysisincluded recall (p=0.007), naming (p=0.044), apraxia (p=0.003), H&Y staging (p=0.046), UPDRS score (p=0.015) and age (p=0.014). At a cutoff value of 6, the 6CIT had a sensitivity of 71.43% and a specificity of 94.43% with an accuracy of 83.93%. Conclusion Cognitive impairment occurs more frequently in patients withPD than in controls. This study also validated the 6CIT as a screening tool for cognitive dysfunction in patients with PD with an accuracy of 83.9%. Key words: Parkinson’s disease, cognition, FePsy, 6CIT, Nigeria, memory.
Résumé Le contexte Arrière-plan La maladie de Parkinson (MP) est une maladie neurodégénérative chronique associée à un dysfonctionnement cognitif entraînant une augmentation du fardeau des soignants et une pression sur les installations de santé communautaire. Objectif Cette étude visait à valider le test de déficience cognitive à six éléments (6CIT) en tant qu’outil de dépistage du dysfonctionnement cognitif chez les patients atteints de MP et à déterminer la fréquence, le modèle et les prédicteurs du dysfonctionnement cognitif chez ces patients. MATÉRIAUX ET MÉTHODES Il s’agissait d’une étude cas-témoins transversale réalisée dans un établissement de santé tertiaire dans le sud-sud du Nigéria. Les performances cognitives de trente patients atteints de MP ont été comparées à trente témoins démographiquement appariés à l’aide de deux batteries de tests neuropsychologiques, à savoir les tests de psychologie du fer (FePsy) et de déficience cognitive à six éléments (6CIT). Résultats La fréquence des troubles cognitifs utilisant le 6CIT chez les patients atteints de MP était de 53% (3,3% pour les témoins). Les domaines cognitifs étudiés englobaient la mémoire, le langage, le dysfonctionnement exécutif, la vitesse psychomotrice et l’apraxie de construction. Les patients atteints de MP ont obtenu de mauvais résultats dans tous les domaines cognitifs de FePsy avec des valeurs p significatives, à l’exception du temps de réaction du choix binaire (p = 0,051) et du tapotement non dominant de la main sur le doigt (p = 0,138). Les prédicteurs indépendants de la déficience cognitive globale chez les patients atteints de MP à l’aide d’une analyse de régression logistique comprenaient le rappel (p = 0,007), la dénomination (p = 0,044), l’apraxie (p = 0,003), la stadification H & Y (p = 0,046), le score UPDRS (p = 0,015) et l’âge (p = 0,014). À une valeur seuil de 6, le 6CIT avait une sensibilité de 71,43 % et une spécificité de 94,43 % avec une précision de 83,93 %. Conclusion Les troubles cognitifs surviennent plus fréquemment chez les patients atteints de DP que chez les témoins. Cette étude a également validé le 6CIT en tant qu’outil de dépistage du dysfonctionnement cognitif chez les patients atteints de MP avec une précision de 83,9%. Mots-clés : Maladie de Parkinson, cognition, FePsy, 6CIT, Nigeria, mémoire. Introduction Parkinson’s disease (PD) is a chronic delibitating disease, complicated by cognitive dysfunction and associated with increased caregiver burden, pressure on community health facilities and significant mortality (56,4). Most of the data concerning cognitive dysfunction in PD are based on studies done in Europe and North America. There is paucity of data on cognitive impairments among PD patients in Sub-Saharan Africa. Knowledge of the pattern of cognitive dysfunction and predictive factors peculiar to different geographical regions may be important in early identification of this complication and ensuring appropriate channelling of resources into caring for patients with PD. Cognition referes to all mental activities associated with thinking, knowing, remembering and communicating. It eencompasses problem solving, decision making, mental grouping of objects and forming judgements (46). The major classes of cognition include reception (ability to select, acquire, classify and integrate information), memory and learning (which involve information storage and retrieval), thinking (involving mental organization and recognizing the information), and expressive functions (which involve speaking, drawing, writing, physical gestures, facial expressions and movements) (46). The prevalence of cognitive impairments in PD has been reported in several developed countries. A systematic review of 27 studies by Cummings reported an average prevalence of 40%. while Aarsland et al. found the prevalence of cognitive impairments in PD to range between 24 and 31% (14,1). The UKCamPaIGN study obtained a prevalence of 36%, while Muslimovic et al. found a prevalence of 24% in a cohort of newly diagnosed PD patients in the Netherlands(31,54). One of the few studies from the sub-Saharan Africa by Osuntokun and Bademosi found a frequency of 5% but a more recent study by Akinyemi et al reported a frequency of 21.6% (61,4).
The diagnosis and type of cognitive dysfunction in PD from previous studies were determined with the use of neuropsychological test batteries requiring professionally skilled personnel and were both time consuming and costly. This placed a lot of stress on the patient and administrators of such test batteries. The Six Item Cognitive Test (9,12,16,17,23,43,75), is a very simple test which could be administered by non-professionals in an average time of three to four minutes. It is a reliable test which has not been validated in patients with PD in our environment. The dearth of information on the pattern and predictive factors of cognitive dysfunction in sub-Saharan African region prompted this study. Therefore, this study sought to determine the frequency and pattern of cognitive dysfunction amongst patients with PD presenting at a tertiary health facility in south-south Nigeria and compared the performance of the PD patients with demographically matched subjects without PD (controls). In addition, we assessed the contributory roles of patient and disease variables to the development of cognitive impairments in PD patients. This study alsosought to validate the Six Item Cognitive Impairment Test in patients with PD in a resource limited environment. Materials and methods Study site The study was carried out in the Neurology outpatient’s clinic of a tertiary health facility located in the cosmopolitan south-south Nigeria. The health facility is situated in the capital of Edo State and serves as the main referral centre for the state and four neighbouring states. Study population Patients with PD, without diabetes mellitus or hypertension, presenting for treatment on an out-patient basis at the medical outpatient clinic of the hospital. Patients were examined by one of the authors (MO) and clinical diagnosis was made based on the UK Parkinson’s Disease Society(UKPDS) Brain Bank Clinical Diagnostic Criteria(39). Inclusion Criteria for patients
Exclusion Criteria for patients
Inclusion /Exclusion Criteria for Controls Normal healthy individuals who fulfilled the above inclusion criteria except that they did not have features of PD or Parkinsons Syndrome, were recruited from thehospital staff and general population, and they freely volunteered to be part of the study. They were age, sex and level of education matched with PD patients. Sampling technique Patients with features of PD who met the inclusion criteria were recruited consecutively at presentation in the neurology outpatient clinics. Sample size A total of 30 patients were recruited for the study.The minimum sample size of patients required for the study was 28, calculated based on the Kish method(44). n = z2 pq = 1.962 x 0.0006 x 0.9994 = 28.44 d2(0.009 )2 n = the desired sample size ( when population is greater than 10,000 ) z = the standard normal deviation, usually set at 1.96, which corresponds to the 95% confidence level p = proportion of patients with PD estimated at 59 per 100,000(8,20,21) q = 1- p d% = absolute deviation from p% that will be tolerated ( i.e. p% give or take d% ) Study design Recruited PD patients with age-, sex-, and level of education-matched controlsreceived clinical assessment using standardised questionnaires to document demographic information and disease related variables including primary language used and reading abilities, level of education, medical history and psychiatry history. A detailed neurological examination was performed on all patients to verify the clinical diagnosis of PD. The stage and severity of the disease were determined using the Hoehn and Yahr staging scale and motor subscale from the Unified Parkinson’s Disease Rating Scale(UPDRS) (38,27). The duration of the disease was defined by the period between the onset of the first symptom as reported by the patient and the time of clinical assessment. Cognitive performances of recruited study participants (PD patients and controls) were assessed with the Six item Cognitive Impairment Test(6CIT) (9), and a computer-based cognitive instrument, the Iron Psychology (acronym-FePsy) (73,58). All the questionnaires were in English language as most people in the locality speak English. The 6 CIT tool The Six Item Cognitive Impairment Test is a simple test which can be administered in three to four minutes. The 6CIT was developed in 1983 by regression analysis of the Blessed Information Memory Concentration scale (BIMC)(9,43). It is an abbreviation of the latter. It is brief, simple, easy to perform and can be translated linguistically and culturally. It correlates well with the MMSE and even outperforms it in milder cognitive dysfunction. Since it is less time consuming, it could be suggested that it is superior to the MMSE. It consists of a total of six questions meant to test memory, orientation and concentration. The total duration of the tests is short; about 3-4 minutes. It uses an inverse score and questions are weighted to produce a total out of 28. Scores of 0-7 are considered normal while 8 and above are cognitively impaired. The 6CIT has been validated in several published studies(9,12,16,17,43).An advantage of this test is its high sensitivity without comprising specificity even in mild dementia. The 6CIT has a positive predictive value of 100% and a negative predictive value of 83.33%. The 6CIT has been validated among Nigerian patients with chronic kidney disease(23) but no validation study has been carried out among patients with PD in Nigeria or other West African countries. Astudy for validation of its use was therefore carried out prior to the main study. The name and address “Amen Bazuaye, 10 Lawani Street, Benin” was used as a substitute for the traditional but foreign “John Smith, High Street, Bedford.” The Iron Psychology (FePsy) In 1978 C.H.W. Van Ziji developed the Iron Psychology (Fepsy), which is a system for automated neuropsychological testing. It is a powerful, automated menu-driven neuropsychological computerized test battery (73) that covers arousal, short term memory, mental speed and vigilance. It contains a set of computerized tests for cognitive functions and a relational database system for storage of the results; each subject undergoes computerized testing to assess cognition (59,5). These test items include: (1) Simple reaction time tasks (auditory reaction time and visual reaction time) which assess mental speed. (2) Binary choice task assesses complex mental speed and concentration. (3) Recognition tasks (simultaneous recognition of words, simultaneous recognition of figures, serial recognition of words, serial recognition of figures) which test for memory. (4) Tapping task which tests motor speed. (5) Vigilance task: this task assesses attention. (6) Corsi’s and Binnie’s Block tapping task: for abstraction, concentration and attention. (7) Computerized visual scanning task (CVST): for assessment of brain damage, abstraction, attention, concentration and mental speed. (8) Rhythm task: this tests memory. (9) Classification task: tests for abstraction. (10) Visual half field tasks: this assesses concentration and includes recognition of words, recognition of figures, matching of lateral words and matching of central words (19,22,35,68). Ethical consideration Ethical approval was obtained from the institutional Ethics and Research Committee before proceeding with the study. Informed written consent was obtained from patients and controls or a reliable relation before recruitment after proper explanation of the study procedure. Recruited study participants were compensated with transport allowance. Statistical analysis Data were analyzed using the Statistical Package for Social Sciences version 16.0 (SPSS) (70).Demographic characteristics of cases and controls were compared using the Student’s t-test for continous variables, while categorical parameters were analyzed using Chi-squared test. Clinical characteristics of cases were summarized using the mean and standard deviation (SD). Cognitive performances of cases and controls were compared using the Student’s t-test, whereas independent predictors of cognitive dysfunction were identified using odds ratios (ORs) from logistic regression models. The confidence interval was set at 95% and a p-value of 0.05 or less was considered statistically significant. RESULTS Determination of cut-off score on the cognitive tool and validation assessment The mean age for the patients was 50.9 (SD 18.59) years, while that of the controls was 51.5 (SD 12.26) years, with no significant difference (t=0.0908; p=0.929). The patients comprised 5 males (50%) and 5 females (50%), likewise the controls. The level of education distribution for both groups were also same: 2 with primary education (20%), 4 with secondary (40%) and 4 with tertiary education (40%). The mean total error scores for the controls and patients were 1.67 (SD 2.06; range 0-6) and 13.7 (SD 8.47; range 4-28) respectively, with a statistically significant difference (t=4.364; p=0.0004) using the 6CIT. By implication, the total correct score followed the reverse pattern with mean scores of 26.33 (SD 2.06; range 22-28) and 14.3 (SD 8.47; range 0-24). The receiver operating characteristic curve (Figure I) was obtained for the total error scores to determine the cut-off score that corresponds to the optimal sensitivity and specificity values for the 6-item cognitive tool. The optimal cut-off score of 6 was obtained with a sensitivity of 71.43% and specificity of 96.43%. The accuracy of the 6CIT tool was 83.93%. This cut-off score was same as that obtained by Katzmanet al.9 The area under the curve (AUC) of 0.85 (SE 0.575) was significant with 95% confidence interval at 0.7373 – 0.9629). The cut-off error score of 6 was used for this study. Results of main study Demographic data of patients and controls. Thirty PD patients and age-, gender- and educationally matched 30 controls participated in the study. The means of their ages were 69.10 ± 7.47and 68.73 ± 7.06 years respectively with male preponderance. The demographic data of the PD cases and the controls are summarised in Table III. *Fisher’s Exact Test The male : female ratio was 26 : 4 for both the PD patients and the controls. This is shown in figureII. The mean age for the PD patients was 69.10 ± 7.47 years, while that of the control was 68.73 ± 7.06 years (p=0.846). The highest freguency of 8 (26.7%) was found in those aged 64-68 years, while the least, 3 (10%) each were in those aged 54-58 years and 79-83 years. This corresponded with that of the control with a p value of >0.05 which was not statistically significant. The proportion of patients and corresponding controls in the stratified age groups is shown in Figure III. The level of education of the PD patients ranged from nil formal education (10%) to tertiary level of education (36.7%). Those with primary level of education were about 20% of the studied population while those with secondary level of education constituted 33.3%. This corresponded with that of the control with a p value of >0.05 which was not statistically significant. Figure IV is a graphical representation of the distribution. Clinical characteristics of the patients with PD The highest proportion of PD cases was seen in stages 2 and 3 of the H and Y scale, each comprising 12 (40%) subjects. The lowest proportion was in stage 1 with 1 (3.3%) patient, while stage 4 had 5 (16.7%) patients. Figure V reflects the stages of PD in the population studied. The overall UPDRS score range for the PD patients was 7 – 64, with a mean of 35.23 ± 14.69. The scores for the males ranged between 7 and 64 with a mean of 35.15 ± 14.25, while those of the females were higher ranging between 22 and 64 with a mean of 35.75 ± 19.81. Table IV reflects the UPDRS rating of the PD patients. Cognitive performance among patients with PD and control subjects on FePsy The patients with PD performed poorly in all cognitive domains of FePsy except the binary choice reaction time and non-dominant hand on finger tapping when compared with the controls. The results of their performances are presented in Table V. The performance of the PD patients on 6CIT was significantly affected by age group (p=0.014), being worse with increasing age, and the UPDRS score being worse with higher scores. However, performance was not significantly affected by H&Y stage, nor disease duration with P values > 0.005. The result is presented in Table IX . PD cases with higher UPDRS scores were impaired with higher scores on the 6CIT being an inverse scoring system with a p value of 0.001 which was statistically significant. The box plot in Fig XI shows the relationship between patients performance on 6CIT and their UPDRS score. The PD patients with longer disease duration were impaired on the 6CIT, however this was not statistically significant at a p value of 0.205. This relationship is shown in Figure XII. The poor performance of PD patients on 6CIT corresponded with lower scores on apraxia. This was significant with a p value of 0.049. This is shown in Figure XIII. The PD patients had worse performance on 6CIT with increasing age. However, this was not significant statistically at a p value of 0.194. This is shown in Figure XIV. Performance on the 6CIT was worse for the PD patients compared with controls, however this was not statistically significant at a p value of 0.114. This is represented in Figure XV. Discussion Demographic data of the patients with PD Thirty PD patients participated in this study. The patients were age-, gender-, and educationally- matched with controls to allow unbiased comparison of results. The mean age of the patients was 69.10 ± 7.47 years with a range of 64-78 years. This may be due to the fact that PD is rare before the age of 50 years with a sharp increase in incidence after the age of 60 years (18,26). Majority of the patients that presented during this period were males and this is consistent with earlier studies that have reported a higher prevalence of PD in men than in women (8,13,28,50,53,57,60). The Hoehn and Yahr staging of the patients ranged from 1 to 4 with most patients in stages 2 and 3. This may be due to the fact that most patients with PD do not present early probably due to lack of impairment in activities of daily living in the early stage of the disease and in the late stage a number might have died either from complications of the disease or other age related illnesses hence the majority of patients were within the middle stages of 2 and 3. Frequency of cognitive impairment in PD The PD cohort studied had significant cognitive impairment as demonstrated in their performances on all the neuropsychological tests used. This is similar to findings in previous studies on cognitive impairment in PD. The frequency of cognitive dysfunction in the PD patients was 53.3% using the 6CIT. This is higher than those obtained in other studies, Cummingsobtained an average prevalence of PD dementia of 40% in a review of 27 studies, while Aarsland et al. in a systematic review found the prevalence of PD to range between 24-31% (14,1). The UK CamPaIGN study obtained a prevalence of 36%, while Muslimovic et al. found a prevalence of 24% in a cohort of newly diagnosed PD subjects in Netherlands (31,54). Osuntokun and Bademosi found a frequency of 5% in a study in Ibadan, however Akinyemi et al had a frequency of 21.6% (61,4). The variation in prevalence of PD from these studies may be attributed to differences in methods of cognitive assessment, operative definition and the study population (24). This study was however on cognitive impairment and not just dementia alone. Pattern of cognitive impairment in PD The 6CIT assessed memory alongside attention and concentration, and orientation. The computer based neuropsychological tool Fepsy assessed memory, reaction time and motor speed. The overall performance of patients with PD on the test instruments was significantly worse when compared with the performance of the healthy subjects. The patients overall performance in the memory cognitive domain was poor compared with the controls. Memory deficit in PD is more a problem of retrieval of coded information than a deficit of registration, encoding and storage of information (56,48,66). This was demonstrated in this study by the performance of the PD subjects in the address registration, recall, and overall memory score. Their performance was worse than that of the controls. Language deficits have been well described in PD and these include naming difficulties, decreased information content of spontaneous speech, impaired comprehension of complex sentences, as well as verbal fluency (7,63). These were exhibited in our cohort of subjects. Confrontational naming defects exhibited by our subjects may be as a result of direct neuronal degeneration associated with hippocampal and limbic deposition of Lewy body pathology in PD (11). However, in many described language deficits, the anatomical regions of the brain responsible for language function are not primarily affected by the disease process, rather they may be related to the dysequilibrium syndrome that characterises PD (25,69). In addition, patients with PD may develope a limbic or hippocampal type of amnesia similar to that seen in Alzheimer’s disease. Such subjects are those in whom AD and PD co-exist or those with AD type pathology (15). The patients with PD performed worse than the controls in the tests assessing executive dysfunction such as the comprehension-motor response. The timed test offers some quantitative measure of the speed of cognitive processing (reduced in PD). PD patients are impaired in tasks requiring the spontaneous elaboration, maintainance and change of cognitive strategies (10,30,36,52,71,76). The dorsolateral pre-frontal cortex has a crucial role in self-directed planning of behaviour and is central to frontal/executive functioning. It’s dysfunction in PD has been alternatively attributed to the disruption of the ‘‘Complex Loop’’ linking pre-frontal to basal ganglia or damage to the ascending dopaminergic mesocorticolimbic pathway (71,41). Some authors however have emphasised the possible role of non-dopaminergic lesions involving cholinergic and noradrenergic systems (65,64,32). Hence, cognitive dysfunction in PD may result from multiple neurotransmitter deficits including dopaminergic, cholinergic, serotoninergic, and noradrenergic systems (25,3,49). According to Fanna et al (29), the dysfunction of the “Complex Loop” would be combined with damage to the “Motor Loop”, a functional anatomic circuit connecting the putamen to the supplementary motor area, whose disruption would be responsible for the motor disability. However, another hypothesis attributed the frontal-like neuropsychological abnormalities observed in PD to the loss of dopaminergic neurons in the ventotegmental area; affecting meso-cortico-limbic pathways, causing dopamine depletion in various cortical areas, including the pre-frontal cortex (45,74,67). The IronPsychology (FePsy) was also used in the evaluation of cognition of both patients and controls. This test has been validated in Nigerians which therefore justifiesits use (46). The subsets of FePsy used in the study included the simple reaction time (auditory and visual), the binary choice reaction time, the recognition memory test and finger tapping task. Subtle subcortical cognitive impairments can be detected by the timed tasks characterized by general slowing of psychomotor speed and thought processes. The reaction times for both patients and controls were found to be much higher than the normative values. In the normative study, a desktop with the keyboard resting on the person’s laps was used while in this study; a laptop with component keyboard resting on the table was used. In the latter case, the reaction times were expected to be more prolonged due to the ‘hand – reaching effect.’ This may also have caused a disparity in the word score between the control subjects in this study and the normative subjects. The PD patients performed worse than controls in all cognitive tasks except in the binary choice reaction time where there was no difference, even though the binary choice sensitivity was less in them.There was also no difference in the tapping task involving the non- dominant hand compared with the control. Therefore, patients with PD may be at higher risk of memory impairment and may have general slowing of psychomotor speed and thought processes. However, their concentration abilities may not differ from the general population.Information processing speed refers to the brain’s ability to rapidly process simple and complex information. Activities of daily living require constant information processing, impairment in psychomotor speed and thought processes as demonstrated by the patients could explain the dysexecutive syndrome seen in these patients. The 6CIT assessed the cognitive domains of memory, concentration and orientation ( in time). The patients demonstrated impairment in all three domains tested. Concentration is the ability to focus and sustain attention, while attention is a cognitive function of the brain that enables a person to triage relevant inputs, thoughts and actions while ignoring those that distract or are irrelevant. Attentional deficits were described as an independent risk factor by Taylor et al (72). Memory deficits in PD have been well described (56,41,66) this was demonstrated with the 6CIT in this cohort of PD patients. Predictors of cognitive dysfunction in PD In this study, certain variables were demonstrated to be predictors of cognitive dysfunction. The age- groups correlated positively with 6CIT and this was related to the level of overall cognitive function. Being an inverse scoring system, it means cognitive function worsened with increasing age groups. The Campaign cohort study revealed that age greater than 72years was an independent predictor of cognitive decline in PD patients (78). Age at onset of the disease and disease duration were not found to be predictors of cognitive dysfunction. This is in keeping with Hughes et al. who found no relationship between age at onset of the disease and cognitive decline (40). Aarsland et al. (2) in another study, showed that it is the general effect of age rather than the age of PD onset that contributes most to the incident dementia in patients with PD, while Lyros et al. (51) showed that the cognitive decline in PD patients might be owing to simultaneous effect of age-related and disease associated neuropathology. This was at variance with Akinyemi et al.(4)who demonstrated that older age at onset of PD showed significant association with cognitive dysfunction. Previous studies have shown that the most important clinical predictors of global cognitive decline following correction for age were neuropsychological tasks with a more posterior cortical basis well as a postural instability gait abnormality (non-tremor dominant) motor phenotype at the baseline assessment (72,78,1,42,79,47,6). This study also demonstrated that recall was significant, however was at variance with the previous studies in that gait abnormality was not found to be a significant predictor of cognitive dysfunction. This study demonstrated that greater severity of PD as indicated by higher Hoehn and Yahr stages or higher scores on the UPDRS motor subscales was associated with worse cognitive profile which was in keeping with previous studies (4,54,55,9). There was no significant relationship between years of formal education and cognitive decline. This is in keeping with studies by Akinyemi et al.(4) and Pai and Chan (62) who also found no significant relationship between the the number of years of formal education and cognitive decline in patients with PD. However Glatt et al.(33)and Green et al. (37) found an association between lower educational attainment and cognitive decline in subjects with PD. Comparison of the test instruments Determination of the nature and degree of cognitive impairment in PD requires comprehensive assessment of cognitive abilities including speed of information processing, attention, memory, language (fluency) and executive functions, which are necessary for goal- directed behaviour. There are a wide variety of such cognitive tests including Cognistat, D2 test of attention, digit vigilance test, Halstead-Reitan neuropsychological battery, Kaplan neurocognitive assessment, Luria-Nebraska neuropsychological battery and the Iron psychology (acronym FePsy), a computerized assisted test battery that contains finger tapping test, auditory reaction time, visual reaction time, visual scanning and binary choice tests. Other neuropsychological tests include Wechsler intelligence scale, trail making tests A and B, Stroop test, tests of memory and learning (TOMAL) and technical performance test (77). The six- item cognitive impairment test (6CIT) (9) and the MMSE are further examples. The 6CIT is sensitive for assessing cortical dementia, however has limited coverage of the cognitive domains. The 6CIT assessed memory (short term), orientation (time) and concentration. In assessing existing tests and test batteries for evaluation of cognition, useful tests are those that are rapid, repeatable, highly reliable, not dependent on experts for administration and free of significant re-test effects (34). This favours the 6CIT, however, a drawback for the 6CIT is its limitation in the range of domains assessed. The timed task tests on Fepsy, a speeded test, are sensitive for detecting subtle subcortical cognitive impairments characterised by generalised slowing of psychomotor speed and thought processes. The generalised slowing of psychomotor speed and thought processes contribute to the dysexecutive syndrome seen in patients with PD. Other domains of cognitive function assessed by FePsy include memory (short term, verbal and non-verbal), abstraction, attention and concentration. Being a computer based instrument, it is subject to less administrative bias the 6CIT. This study assessed cognitive function of PD patients using 2 tools; (a) 6CIT assessed for its utility as a screening tool, (b) FePsy subcortical, thereby covering all the cognitive domains both at the cortical and subcortical levels. The cognitive tests in FePsy are essentially ‘timed’ tasks thus revealing the significant deterioration in mental and motor speed which can not be adequately tested with the 6CIT. CONCLUSION This study showed that there is a high frequency of cognitive impairment amongst patients with PD compared to demographically matched controls and this worsens with the stage of the disease on Hoehn and Yahr staging and with increasing UPDRS score. Other predictors of cognitive impairment in the PD patients included age of the patient and recall. The pattern of cognitive impairment seen in these patients included memory, psychomotor speed, complex mental speed and visuoperceptual dexterity. This study also validated the Six item Cognitive Impairment Test (6CIT) as a screening tool for cognitive dysfunction in patients with PD in the Nigerian population. As a cognitive tool, it is brief and simple, can be translated culturally and linguitsically with good probability statistics. Limitations This is a cross sectional study, as a result it may not capture PD patients with more advanced stage of cognitive impairment. This is a common limitation with this type of study design. The use of the FePsy requires some computer literacy on the part of the investigator. This underscores the relevance of the 6CIT tool which is a non-computer based psychometric test in a resource poor setting. RECOMMENDATIONS All PD patients should be screened for cognitive impairment using neuropsychological tests by their health care providers. Cognitively impaired patients may undergo neurological evaluation with social and vocational adjustment or rehabilitation. Most of these PD patients are dependent on others for means of livelihood due to incapacitation by the disease. There is need for support groups such as the Parkinson’s society. Further studies are recommended to increase knowledge of this disease and the impact on the cognitive function of affected individuals. This will help in the management of these individuals. 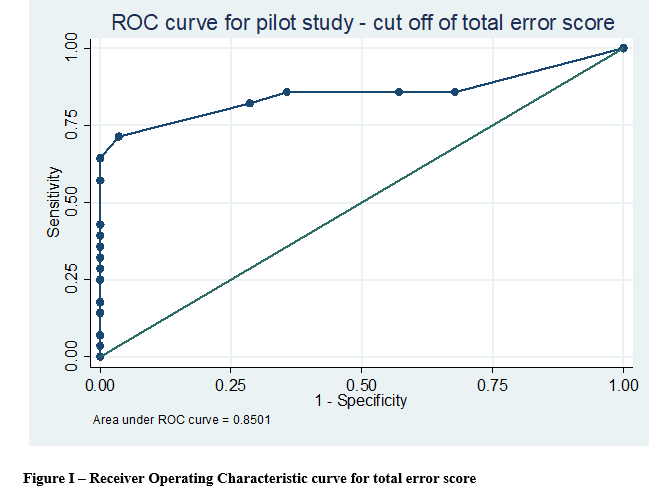 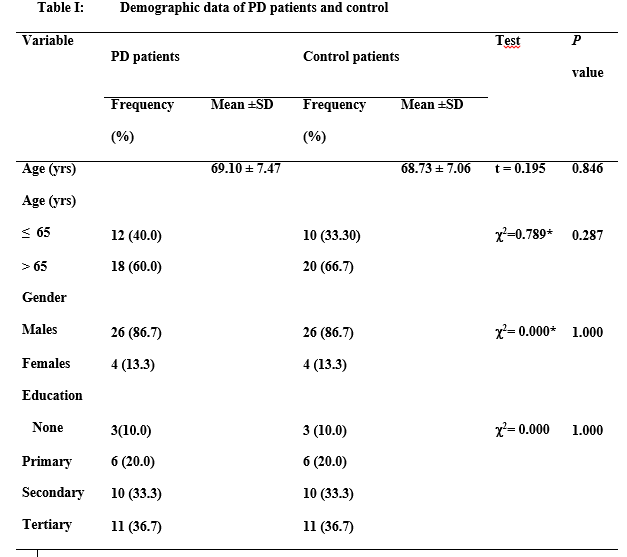 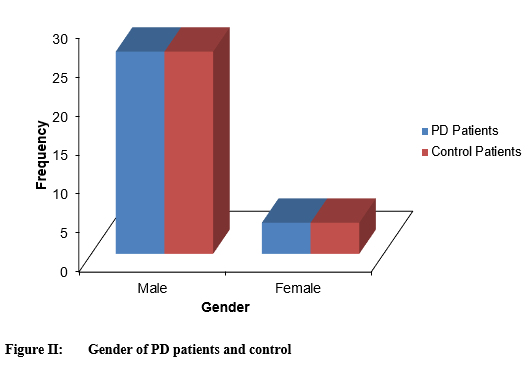 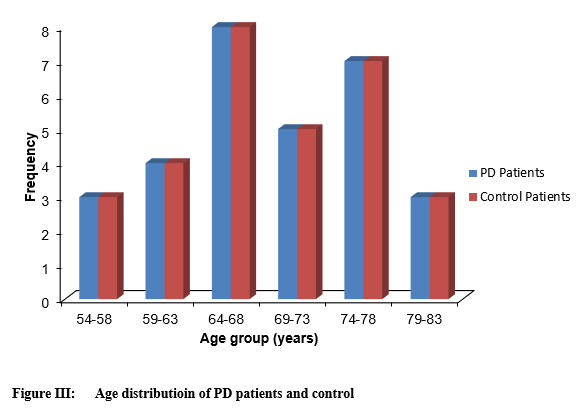 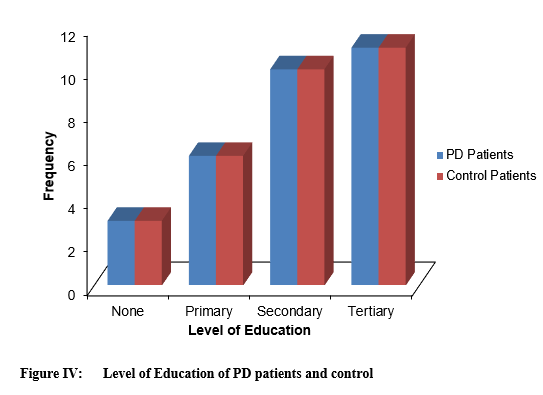 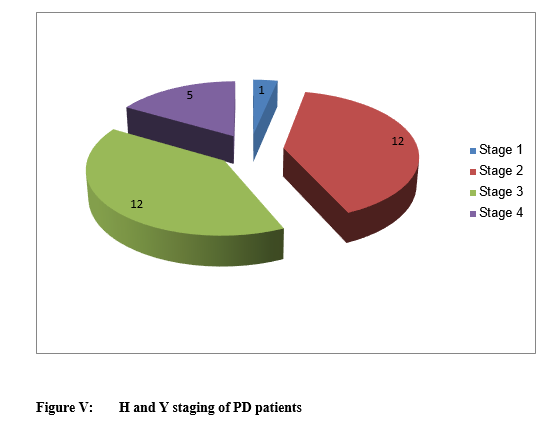 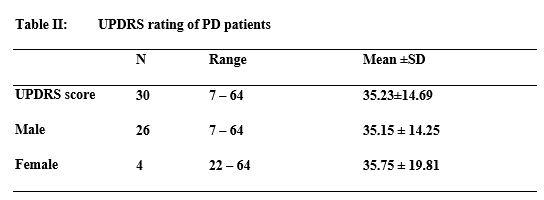 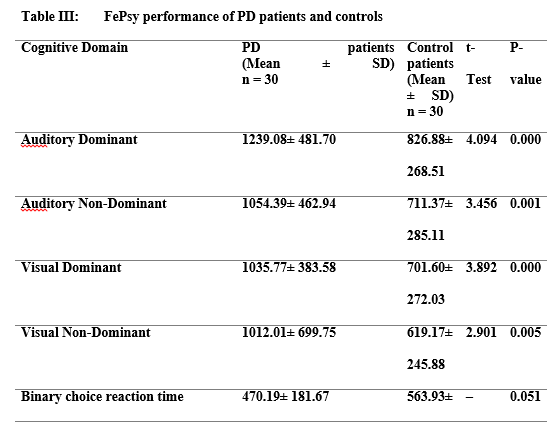 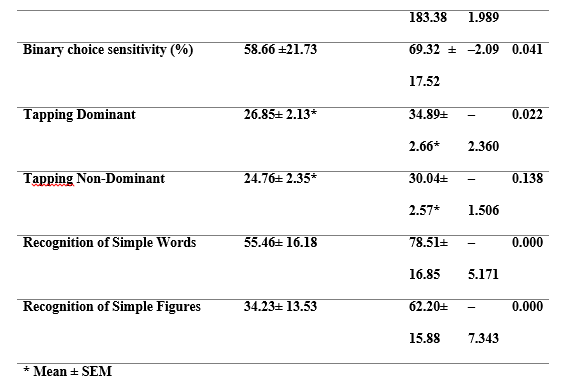 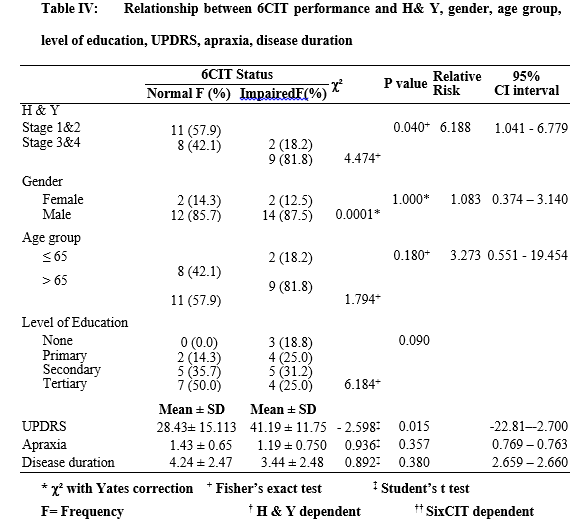 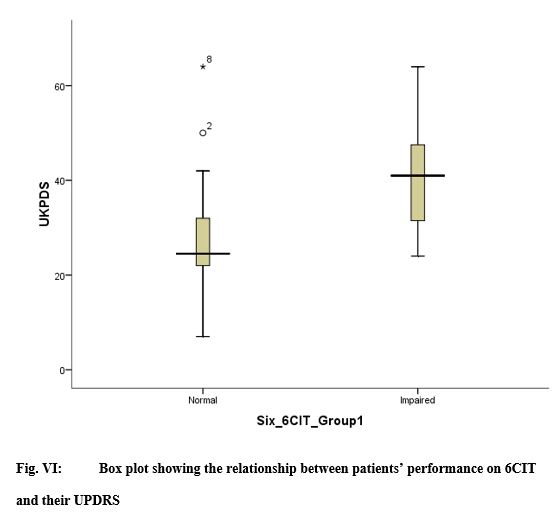 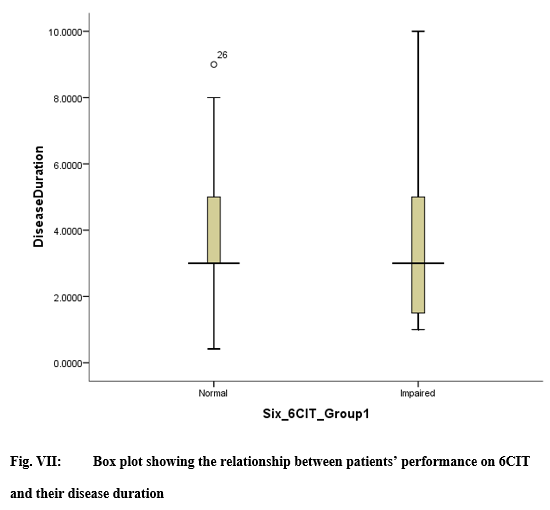 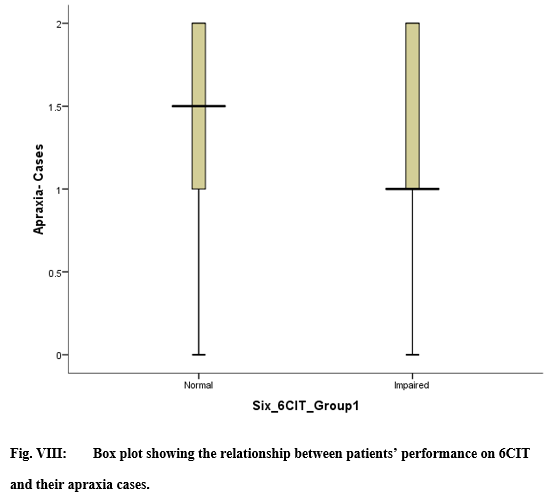 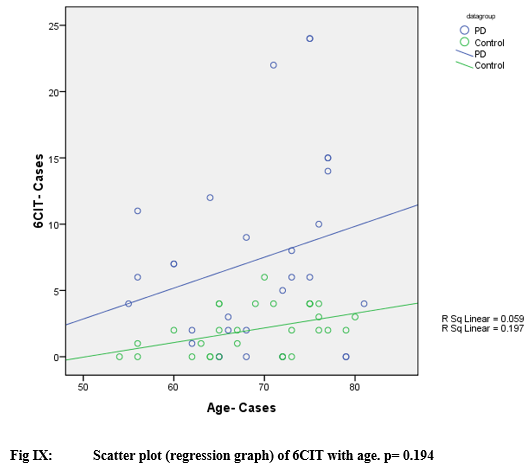 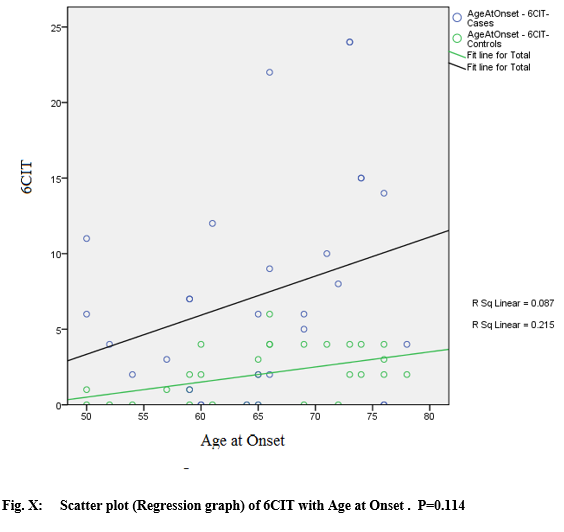 REFERENCES
|
© 2002-2018 African Journal of Neurological Sciences.
All rights reserved. Terms of use.
Tous droits réservés. Termes d'Utilisation.
ISSN: 1992-2647