
|
|||||||||||||||||||||||||||||
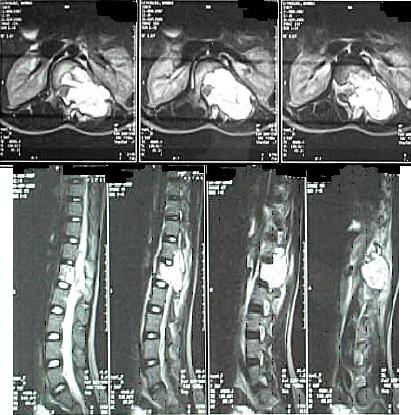
La revue AFRICAN JOURNAL OF NEUROLOGICAL SCIENCES appartient à l’Association Panafricaine des Sciences Neurologiques (PAANS). Le but de la revue est de publier des articles scientifiques abordant tous les aspects des sciences neurologiques. Les articles sont la propriété de la revue. La publication est semestrielle. Les articles soumis, en totalité ou partiellement pour l’essentiel, ne doivent pas avoir été proposés ou publiés dans une autre revue. Thèmes Travaux originaux Les articles doivent être écrits en français et/ou en anglais. Les manuscrits sont examinés par le Comité Editorial et sont soumis à un comité de lecture de manière anonyme. La décision d’accepter ou de rejeter un manuscrit demande un délai de 8 à 10 semaines. Le manuscrit doit être dactylographié en double interligne selon un caractère Times à 12 points. Les manuscrits doivent être dactylographiés sur du papier standard. Les pages sont numérotées en commençant par la page de titre. Le manuscrit doit être signé par l’auteur qui en assume la responsabilité. Il doit en outre certifier que toutes les personnes citées ont lu et approuvé la mention de leur nom dans l’article. Les manuscrits doivent être adressés uniquement à la PAANS par EMAIL à l’adresse suivante: Page 1 : page de titre Le titre doit être écrit en anglais et en français. La page de titre doit contenir le nom complet de chaque auteur, leur affiliation institutionnelle actuelle ; l’adresse complète, le téléphone, le numéro de fax et l’adresse e.mail de l’auteur à qui toute correspondance doit être adressée. Page 2 : résumé Le résumé doit être clair, précis et concis, et ne doit pas comporter plus de 250 mots : Description : Exposer clairement et brièvement le sujet avec un bref rappel des connaissances actuelles. Objectif : Indiquer le but du travail et son importance. Méthode : Décrire les moyens, les techniques avec lesquels l’étude a été conduite. Résultats : Faire part des observations recueillies et présenter les données significatives. Conclusion : Interpréter les résultats. Donner les principales conclusions et recommandations. Proposer d’éventuelles futures investigations. Les mots clés : 3 à 6 mots sur une ligne, en dessous du résumé, par ordre alphabétique. Utiliser les termes tirés de l’Index Médicus : Medical Subject Headings (MeSH). Page 3 : texte Le texte doit être clair, précis et concis. Les abréviations doivent être réduites au minimum et être explicitées dans le texte lors de leur première mention. Les termes anatomiques doivent être ceux de la nomenclature internationale. Introduction : Exposer le but de l’article. Rappeler les connaissances actuelles et les principales références d’articles traitant le sujet. Matériel et méthode : Décrire la méthodologie très clairement. Toutefois il est conseillé de se référer à un travail précédent si la méthodologie y a été rapportée en détail. Ce chapitre doit inclure suffisamment d’informations pour que le lecteur comprenne la méthodologie. La méthode statistique devra être précisée. Résultats : Résumer les résultats observés. Quand une signification statistique est donnée, préciser la méthode utilisée. Donner les valeurs exactes des p ( p < 0,005) Discussion : Insister sur les constatations significatives de l'étude et des investigations. Utiliser éventuellement des sous-titres pour permettre aux lecteurs de suivre la démonstration. Conclusion : Rappeler les principales constatations de l'étude et faire part des implications cliniques et des applications potentielles. Tableaux Les tableaux doivent être présentés sur une feuille séparée et numérotés selon l'ordre d'apparition dans le texte. Chaque tableau requiert un titre et une courte légende. Les abréviations ne sont pas permises. Toutes les mesures doivent être données selon le système métrique international (SI) et indiquées entre parenthèses à travers le texte. Les autorisations de reproduction sont requises pour toutes les illustrations et les tableaux ayant été publiés auparavant. Chaque tableau doit contenir tous les éléments nécessaires à sa compréhension sans avoir besoin de se reporter au texte. Illustrations et photos Les illustrations et les photographies doivent être d'excellente qualité et adresse en JPEG. Les illustrations en couleurs sont publiées à la discrétion du rédacteur en chef. Toutes les illustrations doivent être numérotées selon l'ordre d'apparition dans le texte. Les illustrations doivent être accompagnées d'une brève légende tapée en double interligne, sur une page séparée du texte. Les légendes doivent apporter suffisamment d'informations pour permettre de les interpréter sans se référer au texte. Pour les photographies de personnes susceptibles d'être reconnues, une autorisation écrite doit être obtenue. L'IDENTITE DES PATIENTS DOIT ETRE EFFACEE. La taille d'une image ne doit pas depasser 400 KiloOctet(Ko). Page … : références Les références doivent être dactylographiées, en double interligne sur des pages séparées du texte. La liste des auteurs sera classée par ordre alphabétique.Dans le texte le numéro des références doit être indiqué entre parenthèses par un chiffre arabe. Les références d’un journal doivent inclure tous les auteurs, le titre complet de l’article, le nom du journal abrégé selon l’Index Médicus. Lors de la transcription des références, il n’y a pas d’espace avant ou après les signes de ponctuation du groupe numérique. Vérifiez les références et soyez sûrs qu’elles ont toutes été citées dans le texte. Vérifier également l’ordre alphabétique. Article Book Chapter in a Book : African Journal of Neurological Sciences (AJNS) is owned and controlled by the Pan African Association of Neurological Sciences (PAANS). The AJNS’s aim is to publish scientific papers of any aspects of Neurological Sciences. AJNS is published biannually. Articles submitted exclusively to the AJNS are accepted if neither the article nor any part of its essential substance, tables, or figures has been or will be published or submitted elsewhere. Topics Original Papers Manuscripts may be written in French or/and in English. Manuscripts are examined by the editorial staff and are sent to outside reviewers. Manuscripts are reviewed anonymously. Decisions about acceptable or rejected manuscripts may take within 8 to 10 weeks. The entire manuscript must be typed, double-spaced, with 12 point in the Times font. Manuscript must be sent only by EMAIL to the PAANS at : Page 1 : title page The title should be in English and in French. This title page should contain the full name of each author and their current institutional affiliation ; the complete address, telephone and facsimile numbers, and e-mail address of the author to whom all correspondence should be addressed. Page 2 : abstract The abstract must be clear, precise and concise (no more than 250 words) describing the : Background : briefly describe the problem being addressed and summary of background data. Methods : define the basic design, procedures, and/or setting in which the study was conducted. Results : significant data and observations gathered. Conclusions : Interpret findings and give principal conclusions from the results and recommended guidance pathways and/or need for future investigations. Key Words : – 3 or 6 words – one line below the abstract and listed in alphabetical order. Use terms from the Medical Subject Headings (MeSH) from Index Medicus. Page 3 : text The text must be clear, precise and concise. Introduction : Materials and Methods/Case Material. The Materials and Methods section should include enough details so that the methodology is clearly understood. It is appropriate to refer to previous work if the methodology has been reported in detail; however, this section should include enough information for the reader to gain an understanding of the methodology without referring to previous reports. Results : summarize the findings of the study. When stastical signifificance is attributed, cite the specific method of analysis and use the upper case italic P (P<0.005). Discussion : . concisely emphasize the major findings of the study or investigation . use subheadings so that the reader can follow the authors' train of thought. Conclusions : . restate the major findings of the study or report and . address their potential clinical implications and/or application. Tables Tables should be typed on individual pages and cited in numerical order in the text. Each table requires a title and a short legend. All measurements should be given in System International (SI) metric units, given in parentheses throughout the text. Abbreviations are not permitted in table titles Include written permission from publishers to reproduce any illustrations or tables that have been published previously. Figures Figures are either in black and white line drawings or high quality photographs. Two copies of each figure (each set in a separate envelope) must be submitted. Color figures will be published at the editor's discretion. All figures and tables must be referred to in numerical order in the text. On the back of each figure should be indicated : author's initials, the number. Figure orientation marked by an arrow should indicated the top. Figures should be accompanied by brief legends, typed double-spaced on pages separate from the text. Legends should include enough information to interpret the figure without reference to the text. For photographs of recognizable persons, written authorization from the subject must be obtained. IDENTITY OF THE PATIENTS MUST BE ERASED. The size of a picture must not exceed 400 KiloOctet (Ko). Page … : references Reference numbers in the text should be enclosed in parentheses on the line of type at the citation of the author(s)’name(s) or enclosed in parentheses on the line of type at the ends of sentences. References should be typed, double-spaced, on pages separate from the text numbered consecutively according to the alphabetical arrangement of authors. Article Book Chapter in a Book : ABSTRACT Aneurysmal bone cysts of the spine are benign, highly vascular osseous lesions of unknown origin that may present difficult diagnostic and therapeutic challenges. They are expansile lesions containing thin-walled, blood-filled cystic cavities that cause bone destruction and sometimes spinal deformity and neurological compromise. The treatment of aneurysmal bone cysts of the spine remains controversial according to the literature. We describe a case of a fourteen year old girl with back pain and paraspinal swelling of two weeks duration. Radiological studies revealed an aneurysmal bone cyst which was confirmed by biopsy. Treatment included excision and grafting of the defect with cancellous bone and instrumentation of the deformity. Abbreviations used in the paper: ABC = aneurysmal bone cyst, CT = computerized tomography, MR = magnetic resonance RESUME Les kystes anévrysmaux du rachis sont de nature bénigne. Ils sont richement vascularisés et sont d’origine inconnue posant des difficultés diagnostiques et thérapeutiques. Ces lésions expansives contenant des collections kystiques aux fines parois osseuses peuvent entrainer une destruction, parfois une deformation avec un risque neurologique. Le traitement reste controversé. Keywords : Aneurysmal bone cyst, Spine tumor, kyste anévrismal, tumeur, rachis INTRODUCTION Aneurysmal Bone Cyst (ABC) is a rare localized tumor of the long bones and spinal vertebrae. It was first described by Jaffe and Lichtenstein in 1942 (12). This tumor is found at onset in childhood and early adolescence with a slight preponderance to females (2,7) It constitutes 1.4% of all primary bone tumors and 15% of all primary spine tumors (1,6). It commonly involves the metaphyses of long bones (proximal humerus, femur, tibia) and the flat bones of the pelvis. In the spine it commonly involves the neural arch (20). The cyst is occasionally associated with other tumors of the bone, such as osteoblastoma, osteosarcoma, giant cell tumor and fibrous dysplasia (7,14) and has occasionally been reported to occur at a site of previous trauma to the bone (5). There is tendency towards rapid growth with local expansion, which can exert pressure on an adjacent structure (20). ABC in the spine are generally diagnosed within a few months after the onset of clinical symptoms which include local pain, swelling, muscle stiffness and restriction of movement (15). Rarely in advanced cases does the ABC exert pressure on the spinal cord which can lead to neurologic deficits (17,18,19). Here we describe the diagnosis, management and follow-up of an ABC in a 14 yr old girl. CASE REPORT A 14 yr old girl complained of swelling in the left paraspinal region for a period of two weeks. She also had numbness in the left leg. There was no history of pain or trauma. On examination, the girl was in good general condition. There was a single, fluctuant, tender swelling at the level of T12 in the left paraspinal region. The lower thoracic and upper lumber spine was tender without muscle spasm. Muscle power, sensation and deep tendon reflexes of the lower extremities were normal. Rectal and genital examination were also normal. A complete blood count was normal. An X-ray of the thoracolumbar spine showed destruction of the left pedicle of L1 vertebra with associated paravertebral mass. There was also erosion of the L1 vertebral body. Ultrasonography of the mass suggested a superficial lesion of mixed echogenicity with a fluid level. Spinal computed tomography of the thoraco-lumbar spine showed a mass eroding the posterior elements of the vertebrae at the level of L1 with expansion into the vertebral body of L1 on the left. The lesion was multiloculated, entered the spinal canal and was pressing the cord. A tentative diagnosis of Aneurysmal Bone Cyst was made.  Figure 1  Figure 2
During surgical exploration of the spine at level of T12 and L1, a gray-red fleshy mass 4 cm long with multiple blood filled cysts was found invading the L1 vertebra through the left lamina. The tumor was extradural, attached to the dura but easily separable from it. Cauterization and curettage of the cyst by way of a laminectomy was done. The patient made a good postoperative recovery. Histology of the cyst showed it to be a tumor characterized by spindle cell stroma within which were present a number of dilated blood vessels lined by attenuated epithelium. There were aggregates of giant cells, spicules of osteoid a number of which were calcified.  Figure 4 On follow up at six weeks the girl presented in the casualty with complaints of back pain and pins and needles sensation in both legs. Neurologically the tone, power, reflexes and sensation in the lower limbs were normal. A repeat MRI of the spine suggested residual tumor or recurrence. A second exploration was carried out with curettage of the residual mass. The patient recovered well and was discharged home with intact neurology. A rigid thoraco-lumbar orthosis was tailor made, to be worn when out of bed. At 3 months follow up it was noticed that the patient had developed kyphus deformity at the T9 level. Power in the legs was grade 3. Sensation was intact. X-ray revealed vertebral body collapse with reduction in height of L1 vertebrae.  Figure 5 The patient was operated for T12-L3 spinal fusion with Hartshill rectangle with rib bone grafting of L1 vertebrae. A check x-ray done post-operatively was noted to show malalignment. This appears to have set in during the immediate pre-operative period (prior to date of spinal fusion). A check x-ray just before surgery would ideally have picked this up. The patient’s postoperative follow up course was uneventful and she rapidly regained strength in both legs. She continued to be mobilized with a rigid thoraco-lumbar brace. At 1 yr follow up examination the girl has resumed normal daily activities, is pain free and neurologically intact. She has gradually been weaned off the brace. DISCUSSION An ABC is an uncommon expansile osteolytic lesion of bone consisting of a proliferation of vascular tissue that forms a lining around a blood filled cystic lesion. It is clinically important because it is easily mistaken for a malignancy pathologically in its early to mid-phase. In 20 to 30 % of cases, an aneurysmal bone cyst may be associated with an underlying tumor i.e. osteosarcoma, giant cell tumor, chondrosarcoma, fibrous dysplasia etc (7,14,16). It has been suggested that ABC is not a true neoplasm but rather a vascular malformation. These cysts are generally thought of as a secondary vascular phenomenon superimposed on a preexisting lesion, which presumably initiates a periosteal or intraosseous arteriovenous malformation (1,3,9). The resultant haemodynamic forces generated by high-pressure vascular channels rapidly erode the osseous trabeculae into a cystic cavity. Clinically the patient usually presents with pain and stiffness of the spine. Palpable mass is seen in only 6% of cases. On radiographs the lesion demonstrates loss of pedicle of involved vertebrae (1). The preferred method for evaluation of an ABC is magnetic resonance imaging which can provide as much or more information than a CT scan (4). The differential diagnosis of back pain in children are other tumors of bone such as osteoblastoma, osteoid osteoma, giant cell tumor and fibrous dysplasia. Non-neoplastic causes are osteomyelitis, juvenile rheumatoid arthritis, SLE, Scheuermann disease (16). In our patient the lesion was diagnosed earlier because of presence of localised swelling. However in patients presenting with just low back pain without neurological manifestations or external signs, a high index of suspicion for bony lesion is required and earlier examination, including CT or MRI, should be done. The optimal treatment of aneurysmal bone cysts of the spine remains a subject of controversy. Treatment options for aneurysmal bone cysts have included simple curettage with or without bone grafting, complete excision, embolisation, radiation therapy or a combination of these modalities (20,21). Treatment of ABC with simple curettage can result in obliteration of the cyst (20). Curettage and bone graft has a 20 % recurrence rate, which can be managed with more aggressive curettage or excision (21). If postoperative deformity develops surgical stabilization is indicated (20). The clinical course of aneurysmal bone cysts is sometimes unpredictable and local recurrences have been described after various types of treatments (2). Radiotherapy can also be used effectively in patients who are resistant to surgical treatment or are at high risk for surgery (13). However, possibility of complications such as sarcomatous change, myelopathy, deformation of vertebrae make this mode of treatment less desirable (10). Selective embolisation of the tumor is possible in large tumors that have high risk of bleeding and in places where curettage would be difficult (8). Intra-lesional injection of sclerosing agents is also an effective method for treatment of ABC. Overall cure rates of 87% have been achieved (11). The prognosis of ABC in children is good although there is a high recurrence rate mainly in the 1st year after operation and in patients who undergo partial resection of the tumor (1,2). Therefore these children require careful follow-up and might need additional treatment.
Articles récents
Commentaires récents
Archives
CatégoriesMéta |

© 2002-2018 African Journal of Neurological Sciences.
All rights reserved. Terms of use.
Tous droits réservés. Termes d'Utilisation.
ISSN: 1992-2647