
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
ABSTRACT Background Objectives Methods Results Keywords: Stroke, Quality of life, Sex-differences, South-Eastern Nigeria. INTRODUCTION Measuring health-related quality of life is not only important for quantifying the burden of a disease but also for evaluating the effect of therapies [22]. Evaluation of QOL in stroke populations revealed it as one condition with a multidimensional impact on the QOL of its survivors [3, 14, 20]. This impact may be present even among survivors with mild consequences of stroke and those who may have achieved full independence in Activities of Daily Living (ADL) [1, 4, 13]. Findings from different studies revealed that individual QOL domains may be affected in varying degrees among stroke survivors from different populations. This suggests that environmental or societal factors may also play some role in post-stroke QOL. Factors that may influence QOL in people with stroke include but are not limited to gender [11, 24], depression [4, 14, 21], advanced age [10, 21] communicative disorders [13], cognitive impairment [13, 15, 21] and aphasia [21]. Others are physical disability, [13, 21], poor functional status [10] isolation and diminished social activities [2, 4, 21]. Identifying any factor that may be associated with QOL among stroke survivors in a given population may be crucial to enhancing and ensuring optimal care for individual survivors within that population. Studies from different populations on sex-differences in stroke have been rather contradictory [7, 11, 20, 21], making it necessary to investigate this attribute in the context of individual population. Stroke survivors’ QOL have received considerable attention in the developed world but has just been more recently reported in Nigeria [1, 20]. The available reports from Nigeria are mainly from the South-West, one of the six geopolitical zones in a rather multi-ethnic and highly populated country. There is hardly any report from any other region including the South-East. This hospital-based study set out to provide preliminary data on the QOL of stroke survivors resident in South-Eastern Nigeria and also determine whether there would be sex-differences in the different domains of the SS-QOL for study sample. The study hypothesized that there would be significant differences in the QOL of male and female stroke survivors. METHODS AND MATERIALS Participants Participants were volunteer stroke survivors from purposively selected hospitals and also from randomly-selected communities of Nnewi, Anamba State. Inclusion criteria included a single stroke incidence at least two months prior to data collection, ability to comprehend the English language and attending physicians’ diagnosis of mild to moderate stroke. They were recruited from Nnamdi Azikiwe University Teaching Hospital, (NAUTH), Nnewi, Anambra State; Enugu State University Teaching Hospital, Enugu, Enugu State and Federal Medical Centre, Owerri, Imo State. Those recruited from the communities were recruited through adverts placed in church bulletins and community town-criers. Some others were recruited by snowballing sampling technique from contacts made through initial volunteers. Majority of this group of participants had been managed at private health facilities and provided information on diagnosis based on what the attending physician told them. Each participant signed an informed consent form in accordance with the ethical principles contained in the Declaration of Helsinki (1964, revised in 1975, 1983, 1989, 1996 and 2000) of the World Medical Association. Measurement and data analysis Participants’ QOL was evaluated with the Stroke-Specific Quality of Life Scale (SS-QOL). This is a patient-centred outcome measure intended to provide an assessment of health-related quality of life specific to patients with stroke. It is a self-report scale containing 49 items in 12 domains viz: Mobility, Energy, Upper extremity function, Work/productivity, Mood, Self-care, Social roles, Family roles, Vision, Language, Thinking, and Personality. Items are rated on a 5-point Likert scale. One out of three different response sets each with scores ranging from 1 (for total help/ could not do it at all/ strongly agree) to 5 (for no help needed/ no trouble at all/ strongly disagree) is applicable to each of the items. Higher scores for any item or domain indicate better functioning [17]. The internal consistency value is 0.73 for all domains while the test-retest and inter-rater reliability are respectively 0.92 [25]. RESULTS One hundred and three (53 males, 50 females) stroke survivors participated in this study, 55.34% of whom had the hemiparetic lesions on their right limbs. The right limbs were affected in over 64% and 47% of females and males respectively (p=0.12). The average study participant was 62.80±11.46 (range =25.0 to 86.0) years old and had a mean post-stroke period of 14.18±26.76 months at the time of data collection. Average post-stroke period for males (15.89±35.16 months) was not significantly different to that for females (12.38 ± 3.13). Participants in both groups were also matched for age. Participants’ best scores were in the vision, thinking, mood and language domains of the SS-QOL and their worst score was in the social roles domain. Participants’ overall QOL score of 156.71 ± 41.64 could be regarded as fairly good (Table 2). QOL scores were not significantly different for males and females overall and in all the domains (P≥ 0.05). DISCUSSIONS The QOL scores for participants in this study as proportions of the maximum possible scores were well above average overall. Scores in the vision, thinking, mood and language domains were very good but scores in most of the other domains were just about average. There was no significant influence of gender on any of the domains and overall QOL. The fairly high overall QOL score for the participants is in agreement with previous reports [1, 11, 20]. Owolabi and Ogunniyi [20] suggested that QOL may not be severely affected in milder forms of stroke and that acquired coping strategies may minimize the effect of stroke on QOL. Lower scores in the role functioning domains (family roles and particularly social role domains) more than most others suggest that participants judge themselves more poorly when it comes to activities involving interaction with significant others. The expectations of these significant others could have directly or indirectly influenced survivors’ judgment of these aspects of their lives. The observance of lower scores in these domains is in line with that of Hackett et al [11] but contrary to that of Kong and Yang [14]. Both studies used the Short Form Health Survey (SF-36) Questionnaire, a generic scale to assess QOL. Akinpelu and Gbiri [1] and Owolabi and Ogunniyi [20] using different generic and stroke-specific QOL scales respectively found survivors QOL different to that of apparently healthy controls in the community domain but not in the intimacy domains. These domains may be equated to the social role and family roles of the SSQOL. The finding on the other hand may be reflective of participants’ perception of family and community support. The contribution of social support to the health-related QOL of stroke survivors is already documented [19]. This was however not investigated in this study. Organized social support services are not readily available in Nigeria and the pressure of surviving a harsh economic environment is gradually eroding the Nigerian cum African traditional (informal) social support system. The mobility, upper extremity function, work/productivity and self care (Physical functioning) domains were also remarkably affected as scores only ranged between 53 and 62 percent of possible maximum for each domain. Studies have generally reported decline in physical function as the most significantly affected aspect of QOL [1, 11, 14, 16, 20]. The energy domain was just as affected in the sample as the physical functioning domains. The energy (vitality) domain in stroke survivors had been reported not to be significantly different from that of the general population [14, 24]. This study could not establish statistically significant gender difference in QOL among stroke survivors. Previous studies have reported that female stroke survivors have poorer QOL than males [4, 8, 24]. Our findings seem to contradict this, though the scores for female survivors were slightly but not significantly lower in all but three of the QOL domains. The finding of though not-significantly lower scores in the mobility, upper extremity function, self care and work productivity domains may suggest to some extent lower physical functioning in females. This however may reflect pre-stroke differences rather than the effect of stroke. Prestroke physical functioning has been reported to be lower in females [16]. Contrary to our findings, other authors have reported lower physical functioning in women after stroke [8, 16]. Another has even suggested functional recovery post-stroke to be poorer in women [5]. Male survivors have a non-statistically significant higher score in the family role domain which might just be due to females placing more emphasis on these expected roles. The typical Nigerian woman, like her counterparts in some other African and non-African cultures manages the home and organizes things for her spouse and children. She is more likely to feel she is a burden and regards her condition as great interference with her personal life if due to functional limitation; she is hardly able to perform these roles. A similar finding was reported by Gargano and Reeves [8]. Lai et al [16] also reported that men rated better on an Instrumental Activities of Daily Living (IADL) scale assessing activities traditionally performed by women (shopping for groceries, preparing meals etc). The least score for study participants was obtained in the social role domain. There was however no difference in the scores of male and female participants in this domain. This suggests that both sexes may be experiencing similar challenges from a largely inadequate and poorly organized social support system. Lynch et al [18] had earlier reported that social roles are altered significantly when patients can no longer work. Our study participants scored slightly just above average in the work/productivity domain. Real or perceived inability to do productive work may be responsible for the rather poor score in the social role domain. Limitations/ Recommendation This study has certain strength and limitations that ought to be highlighted. First is that the sample comprised survivors attending medical and physical therapy clinics in selected government-owned tertiary health centres and others receiving care at other hospital-types, faith-based clinics and alternative medical practice. Obtained result is thus somewhat representative of stroke survivors from this part of Nigeria. However, survivors with severe affectation and those who could not comprehend the English language were excluded from the sample. These findings could thus not be generalized to such individuals. Also information on stroke diagnosis for participants recruited from the communities was obtained through patients and family sources and not directly from physicians. This information may not be totally accurate. This study however provided for the first time, data on the QOL of stroke survivors from a South-Eastern Nigeria sample, allowing for regional comparison of QOL among different tribes in a multi-ethnic society like Nigeria. The focus of sex-differences in stroke survivors’ QOL has particular importance in Nigeria. This is a country where different cultural demands for both sexes may influence their perception of QOL post-stroke. However our finding of non-significant differences between the two groups seem to suggest that other factors aside sex may be more important in determining survivors’ QOL post-stroke. Another study, though, would be needed to confirm this. Clinicians managing stroke survivors should consider not just the biological differences between the sexes but also other sociodemographic variables. More importantly, our findings of very low scores in the social role domain greatly underscores the importance for governments and communities in developing countries like Nigeria to show greater commitments in the area of social support. Social support services should be made readily available and easily accessible particularly for groups with special needs like stroke survivors. Vocational rehabilitation centres may particularly help to improve QOL in this domain as enhanced ability to work or be productive may increase individual’s perception of well-being. CONCLUSIONS
Table 1: Participants’ Mean Score for Quality of Life at Its Different Domains.
% (MPS) = Percentage of Maximum Possible Score Table 2: Comparison of participants’ mean QOL scores across domains by gender using Mann-Whitney U-test
U= Mann-Whitney U test statistics THE EAST AFRICAN ASSOCIATION OF NEUROLOGICAL SURGEONS 3rd ANNUAL SCIENTIFIC CONFERENCE THE EAST AFRICAN ASSOCIATION OF NEUROLOGICAL SURGEONS 3rd ANNUAL SCIENTIFIC CONFERENCE ISPN KARL STRORZ EDUCATIONAL COURSE WORKSHOP JUNE 2ND -5TH, 2013, NAIROBI, KENYA EAANS 3rd Annual Sci Conf 20.3.13 advanced programme.pdf A SALUTE TO SAYED EL GINDI – AN AFRICAN TITANA SALUTE TO SAYED EL GINDI – An African Titan. The serious practitioners of neurosurgery (brain and spinal cord surgery) in Africa are never put off by adversity. However, the news that came out of Heliopolis, Cairo this week was particularly tough to handle. Prof. Sayed El Gindi came of age when the anti-colonial struggle was gathering strength on the African continent; he completed his undergraduate medical degree from Cairo University in 1956. In the ensuing years, as many African states gained the right to self-determination, he pursued post graduate training in neurosurgery- both in Cairo and the UK and gained the FRCS in 1963. Fully compatible with the ethos at the time, Sayed El Gindi returned to Egypt and established a Neurosurgical Department at the Maadi Military Hospital and powered it into one of the best specialist units in the country. He later went on to assist in the establishment of Neurosurgery Departments in Alexandria, Mansoura and Luxor. The pan-Africanist fervor of the times was not lost on El Gindi. He embraced it with zeal and proceeded to train many neurosurgeons from Africa and the Arab world. His first trainee was Adel El Hakim, a life-long El Gindi loyalist- and an excellent neurosurgeon who rose to become Professor and Head of the Neurosurgery Department of Ains Shams University and later the Nasser Institute. In the academic arena, El Gindi was on the Editorial Board of the flagship scientific journal-“Neurosurgery” and he published over 100 peer-reviewed articles in international scientific journals- all of which have helped to provide knowledge and improve patient outcomes. Whether it was on a boat on the Shire River as the hippopotami saluted us with their glistening sabres; or at a beach side restaurant in Cotounu; or navigating the market stalls in Blantyre and Aswan or standing together and watching the sunset over the west bank of the Sakumono Lagoon- for me he was a quiet re-assuring presence, rooted and confident in his African and Arab heritage- a renaissance man; a true citizen of the world. I still remember poignantly, the tightness of his jaw and the gleam in his eyes when he stood at Kwame Nkrumah’s grave in silent tribute on that Sunday morning barely a few hours after arriving in Accra for the first time; El Gindi never abandoned the Pan-African spirit. As cognoscenti of the arts, he and his life-long partner- Mrs. Samia El Gindi, had an extensive collection of paintings, illuminated manuscripts and objets d’art at their lovely Heliopolis apartment to uplift the human spirit; and their hospitality was always the most gracious. If we are to honor this gentle giant of a man and titan, then we must perpetuate his legacy of live long service and humanism – always bringing living water to a thirsty land. Nii B. ANDREWS, MD  Sayed El Gindy
RESUME Objectif Méthode Résultats Conclusion Mots clés : malformations kystiques, fosse postérieure. ABSTRACT Introduction Material and Method Results Conclusion Keywords: Dandy Walker Complex, Dandy Walker malformation, hydrocephalus, Niger. INTRODUCTION Les classifications et descriptions des malformations kystiques de la fosse postérieure dans la littérature sont basées sur le stade du développement embryologique, la communication ou non avec les espaces sous arachnoïdiens ou le V4, les modifications morphologiques de la fosse postérieure et l’association avec d’autres malformations sus-tentorielles (21). La première description de ces malformations a été rapportée par Dandy et Blackfan en 1914 (12). La triade de la malformation de Dandy Walker date de 1963 par D’Agostino et Hart (11). Cette triade s’associe dans les formes évoluées à une hydrocéphalie (5). D’autres malformations kystiques de la fosse postérieure ont été décrites. Ces descriptions étaient souvent discordantes (21). Sur la base d’étude embryologique (21) et IRM, les travaux de Barkovich et al(3) en 1989, ont apporté des précisions dans la classification des malformations kystiques de la fosse postérieure. Ainsi, la malformation de Dandy-Walker, le Dandy-Walker variant, la mega-cisterna magna, le kyste de la poche de Blake, le kyste de la valecula représenteraient des stades d’évolution malformative dans la fosse postérieure avec une base embryologique commune (21). Le Dandy Walker complex représenterait le stade tardif de ces malformations. Cette étude a pour objectif la description des aspects épidémiologiques, cliniques et scannographiques des malformations kystiques de la fosse postérieure chez l’enfant et l’évaluation des indications et résultats du traitement par dérivation ou par endoscopie. METHODE Il s’agissait d’une étude prospective réalisée dans le service de neurochirurgie de l’hôpital national de Niamey (Niger) entre janvier 2007 et février 2012. Etaient inclus, les enfants de 0 à 5 ans sans antécédent de méningite admis pour une macrocranie ou un retard psychomoteur et dont le scanner a révélé une malformation kystique de la fosse postérieure. Pour chaque enfant étaient analysés, les antécédents familiaux, néonataux et le statut clinique. L’évaluation psychomotrice était réalisée avec l’échelle de développement de Gezel-Lezine. Les patients avec un quotient de développement inférieur à 60 sur cette échelle étaient exclus de l’étude du fait de la dégradation de leur état général. Une description scannographique de la malformation kystique et des anomalies sus- tentorielles était réalisée. En l’absence d’hydrocéphalie une dérivation kysto-péritonéale était réalisée seulement lorsque que les signes de souffrance de la fosse postérieure étaient évidents et récents. En présence d’une hydrocéphalie, un traitement endoscopique était réalisé en première intention comprenant une VCS large (figure11), une coagulation du plexus choroïde autour du foramen inter-ventriculaire droit et de la corne temporale droite selon la taille ventriculaire. Lorsque le kyste de la fosse postérieure était situé en sus-tentoriel une mise en communication de ce kyste avec le ventricule latéral (VL) était réalisée après la VCS. La découverte endoscopique de fausses membranes et d’arachnoïdite était un critère d’exclusion de l’étude. La cotation des facteurs prédictifs des résultats de la VCS selon Warf (6) était utilisée pour certains patients à titre de test avant son application systématique dans le service. Cette cotation comprend des critères d’âge (≤ 6mois = 0 ; entre 6mois et 1 an = 1 ; ≥ 1an = 2), des critères étiologiques (myéloméningocèle = 2 ; infectieux = 1 et autre = 0) et des critères de coagulation des plexus choroïdes (complète= 2 ; partielle= 1 et absente = 0). Les patients ayant une chance élevée de succès ont un score entre 7 et 9 ; ceux avec chance modérée de succès ont un score entre 3 et 6 et ceux avec une faible chance de succès ont un score entre 0 et 2.
Etaient exclus de l’étude les patients n’ayant pas été suivis pendant au moins 6 mois en post- opératoire. L’antibioprophylaxie était poursuivie en post opératoire pendant 7 jours à base de ceftriaxone injectable. Une fontanelle tendue et non affaissée à 1 mois post-opératoire était considéré comme un échec et une dérivation kysto-péritonéale était réalisée. Une réduction de l’index de Evans entre 0,06 et 0,1 à 6 mois post-opératoire était considérée comme une stomie efficace. RESULTATS Entre janvier 2007 et février 2012, 1300 scanners cérébraux ont été réalisés chez les enfants de 0 à 5 ans à l’hôpital national de Niamey soit une moyenne de 5 scanners par semaine. L’indication du scanner était essentiellement la macrocranie et le retard psychomoteur. Une malformation kystique de la fosse postérieure a été retrouvée dans 144 cas soit 11,076% des cas. La série comportait 84 garçons (58,33%) et 60 filles (41,66%) avec un sexe ratio de 1,4. La moyenne d’âge était de 8,7 mois (7 jours – 5 ans). Il s’agissait de nouveaux- nés et nourrissons de moins de 12 mois dans 76 cas (52,77%), d’enfants de 1 à 3 ans dans 41 cas (28,47%) et de 3 à 5 ans dans 27 cas (18,75%). Les grossesses étaient à terme 8- 9ème mois dans 128 cas soit (88.88%). On notait des antécédents familiaux de spina bifida, d’hydrocéphalie ou de mariage consanguin dans 28 cas (19,44% des cas). Une maladie maternelle au cours du premier trimestre de la grossesse était rapportée dans 23 cas (15,97% des cas). L’accouchement était par voie basse dans 127 cas (88% des cas). Une souffrance néonatale était notée dans 37 cas (25,69% des cas). Une macrocranie était rapportée à la naissance par les mères dans 62 cas (43,05%). A l’admission, la moyenne des périmètres crâniens était de 48,33 cm ; la moyenne des QD était de 81,84 et 63,19 % des patients avaient une importante ventriculomégalie: Evans ≥ 0.4. La moyenne de l’index d’Evans pré- opératoire était de 0.423. La série comportait 144 patients porteurs de kyste de la fosse postérieure. Il s’agissait de 67 cas de malformation de Dandy Walker (46,52%), de 21 cas de Dandy Walker variant (14,58%) et de 56 cas de kyste de la fosse postérieure considérés comme megacisterna magna ou kyste de la valecula ou Dandy Walker complex (38,88%). Un seul cas en faveur d’un kyste arachnoïdien a été identifié associé à des malformations kystique et parenchymateuse sus tentorielle pour lequel aucun traitement chirurgical n’a été retenue (figure 9). Sur les 144 patients porteurs de malformation kystique de la fosse postérieure l’hydrocéphalie était associée dans 128 cas soit dans 88,88% des cas. Le quotient de développement (QD) selon Gezel et Lezine était supérieur à 85 dans 35,41% (51 cas), intermédiaire entre 60 et 85 dans 49,30% (71 cas) et en dessous de 60 dans 15,27% (22 cas). La cotation prédictive des résultats post- opératoire de Warf a été utilisée chez 22 patients : 7 patients avaient une chance élevée de succès (7-9 points), 11 avec chance modérée de succès (3-6 points) et 4 patients avec une chance faible de succès (0-2 points). L’indication opératoire a été retenue chez 77 enfants (53,47%) suivis pendant au moins 06 mois dont 8 n’avaient pas d’hydrocéphalie (5,55%). Il s’agissait de 49 cas/ 67 de malformation de Dandy Walker, de 7 cas/21 de Dandy Walker variant, et de 21 cas/56 retenus comme des megacisterna magna ou de kyste de la valecula ou Dandy Walker complex. L’indication opératoire n’a pas été retenue dans 67 cas soit 46,52%. Concernant la malformation de Dandy Walker et le Dandy Walker variant, l’indication opératoire n’a pas été retenue (56 cas/88 soit 63,63) du fait de la dégradation de l’état psychomoteur des enfants en relation avec probablement l’évolution tardive de l’hydrocéphalie. L’âge moyen de ces enfants non opérés était de 15,87 mois. Pour les cas de megaciterna magna l’indication opératoire a été retenue dans 21 cas/ 56 (37,5%) devant un syndrome de la fosse postérieure associée ou non à une hydrocéphalie. Pour les autres cas (62, 5%), il s’agissait de découverte fortuite ou avec des troubles psychomoteurs mineurs ou en relation avec des anomalies sus- tentorielles. Le syndrome de la fosse postérieure chez le nourrisson se manifeste dans cette série par une régression des acquisitions motrices segmentaires et axiales avec au scanner une malformation kystique de la fosse postérieure sans hydrocéphalie (figures 1, 2, 3). Chez les grands enfants de cette série à côté des régressions des acquisitions motrices, sont rapportés par les mères une régression intellectuelle. Cette régression intellectuelle avec parfois des troubles de comportement est souvent le motif de la consultation. C’est souvent dans ces cas que l’on découvre au scanner une megacisterna magna communiquant avec le V4, sans atrophie cérébelleuse évidente sans modification du tronc cérébral sans anomalie sus- tentorielle évidente. Aucune indication thérapeutique n’était retenue dans ces cas. (Figures 4 et 5). Notre endoscope rigide nous permettait seulement la visualisation de l’orifice supérieure de l’aqueduc ainsi que les récessus de la paroi postérieure du V3. Ces récessus étaient dilatés 42,02% (29 cas sur 69) ce qui apparait comme un signe de sténose de l’aqueduc. Aucune exploration endoscopique de l’aqueduc du mésencéphale n’a été réalisée au cours de cette étude. La coagulation des plexus choroïdes a toujours été partielle. Dans 42,02% des cas (29cas / 69), la technique endoscopique était un échec avec une fontanelle non affaissée et tendue à la consultation de contrôle à 1 mois pour 17 cas ; échec également pour 8 cas entre 1 à 3 mois (alors que la fontanelle était souple lors de la consultation précédente) et pour 4 cas entre 3 à 6 mois. Aucune complication per- opératoire ni d’infection post-opératoire n’ont été observées. Deux décès étaient rapportés au 4ème et 5ème mois dans un tableau de bronchopneumonie et d’hyperthermie. Parmi les patients ayant une cotation prédictive élevée de succès (7 cas), la technique était un succès dans 6 cas ; les patients ayant une cotation intermédiaire (11 cas), la technique était un succès dans 6 cas. Pour les patients ayant une cotation faible de succès (4 cas), la technique était un échec dans tous les cas à 1 mois. Le suivi moyen était de 16,4 mois (6 mois – 59 mois) avec au moins un scanner de contrôle après 6 mois post- opératoire. Le taux de succès du traitement endoscopique seul était de 57, 97% (40 cas / 69) à 6 mois avec des enfants de plus de 12 mois pour près de la moitié des cas. Il est basé sur la réduction du périmètre crânien, l’affaissement de la fontanelle, l’amélioration du QD, et la réduction du volume ventriculaire par l’index d’Evans à 6 mois pour les patients avec hydrocéphalie. La réduction moyenne des périmètres crâniens était de 2, 45.cm à 6 mois. La réduction moyenne de l’index d’Evans était de 0, 0735 à 6 mois. Le gain moyen du QD à 6 mois était de 8,79 points. DISCUSSION Plusieurs classifications et descriptions des collections du liquide cérébrospinal de la fosse postérieure sont rapportées dans la littérature (10,11, 24, 21) Pendant longtemps plusieurs termes étaient utilisés pour indiquer la même pathologie ou un seul terme était utilisé par différents auteurs avec diverses interprétations (21) Dandy et Blackfan en 1914 (10) décrivaient une énorme dilatation kystique du V4 avec déplacement antérieur du vermis attribués à une atrésie primitive des foramen cérébelleux. Benda (5) en 1954 rapportait que l’atrésie des foramen latéraux et médian du V4 n’était pas le seul facteur pathogénique et introduisait le terme de malformation de Dandy Walker. Les études embryologiques et IRM (3, 21) apportent des clarifications dans la description des malformations kystiques de la fosse postérieure. Le point de départ de ces malformations serait un arrêt dans le développement du rhombencéphale entre la 7ème et la 10ème semaine embryonnaire avec défaut de fusion des lèvres rhombiques sur la ligne médiane. Ceci a pour conséquence la persistance à cette hauteur de la lame basale entrainant la malformation du vermis et du V4, la migration crâniale du plancher du V3 et l’arrêt de la migration caudale du sinus droit (21). Dans les cas de malformation de Dandy Walker, de Dandy Walker variant, de mega cisterna magna ou de Dandy Walker complex associés à une hydrocéphalie la technique était une VCS associée une coagulation partielle des plexus choroïdes ainsi qu’une fenestration du kyste dans le VL. Dans la littérature, Mohanty rapporte 21 cas de Malformation de Dandy Walker et de Dandy Walker variant traité par endoscopie dont 16 par VCS seule, 3 par VCS+ stent et 2 par VCS+ fenestration du kyste. Ils rapportent un taux de succès de 76% (18). D’autres études ont également rapportées des taux de succès similaires à 74% (11) et à 93.3% (13) Les critères prédictifs de Warf utilisés dans 22 cas de cette série ont été concluants dans 80% des cas. Ces résultats doivent être complétés par une série plus grande et doivent être interprétés en tenant compte de la réalisation des larges stomies sur le plancher du V3. Notre taux de succès avec VCS, coagulation partielle plexuelle et fenestration était de 57.97% des cas à 6 mois. Ce taux tout en étant moins important que celui d’autres auteurs encourage cependant à mieux définir les indications du traitement endoscopique pour éviter sa systématisation dans le traitement des hydrocéphalies. CONCLUSION La VCS associée à une coagulation partielle des plexus choroïdes et une fenestration du kyste peut être une option thérapeutique dans la prise en charge des malformations kystiques de la fosse postérieure avec hydrocéphalie.  Figure 1, 2  Figure 3  Figures 4 ,5  Figure 6  Figures7, 8  Figure 9  Figure 10  Figure 11 Tableau I: Evaluation pré et à 6mois post op de 22 patients selon la cotation de Warf B.
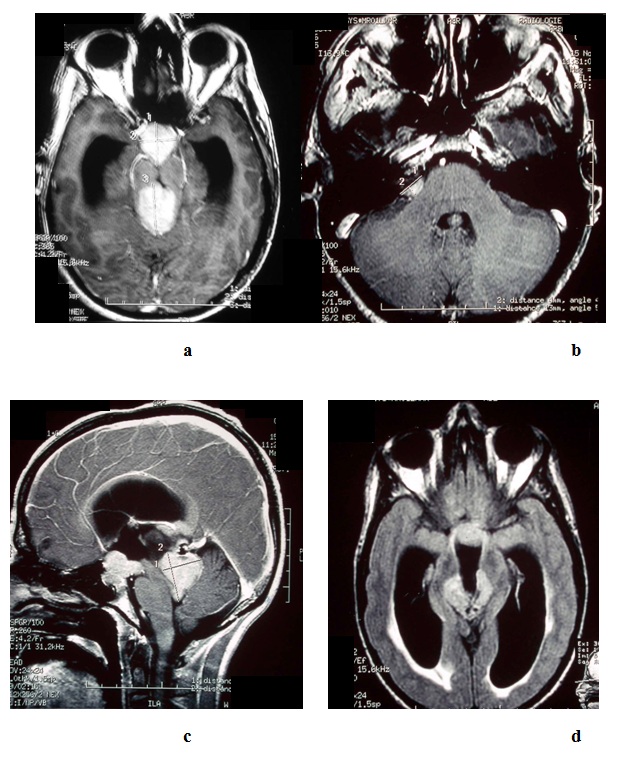
ABSTRACT Germinomas are malignant tumors arising from primitive germ cells. They may be solitary or multiple and can be situated along the midline structures or in other intracranial regions. We report on one case of multiple intracranial germinoma. A 38 year-old male patient presented with signs of increased intracranial pressure and bilateral dimunition of visual acuity. A brain MRI showed multiple lesions at the level of the pineal region, the suprasellar region and in the right pontocerebellar angle. Tumor markers were positive. He underwent radiation therapy and chemotherapy with good recovery. To the best of our knowledge no similar case was described in the African literature before. Key-words: Germinoma – Brain – Suprasellar – Pineal region RESUME Les germinomes sont des tumeurs malignes dérivant des cellules primitives germinales occupant les structures de la ligne médiane au niveau cérébral telle la région pinéale et/ou sellaire. Nous rapportons un cas de localisation multiples chez un patient de 38 ans, révélé par un syndrome d’hypertension intracrânienne et une baisse de l’acuité visuelle.L’IRM cérébrale a permis de voir les trois localisations: pinéale ; sellaire et au niveau de l’angle ponto cérébelleux droit .Les marqueurs tumoraux étaient positives. Le patient a bénéficié d’un shunt interne et a entrepris aussitôt un traitement complémentaire enchainant chimiothérapie et radiothérapie avec une très bonne évolution clinique et radiologique.A notre connaissance aucun cas similaire n’a déjà été décrit dans la littérature africaine. Mots clés: Germinome – cerveau – suprasellaire – région pinéale INTRODUCTION Germinomas are primitive malignant tumors, arising from neural germ cells. They represent about 2/3 of intracranial germ-cells tumors (1, 2, 3), and about 2% of intracranial tumors. They are very frequent in Japan (4, 5, 6). The most common location for germinomas is the pineal region, but they may occur along the midline structures for example: the suprasellar and basal ganglia. Germinomas can also occur as multiple lesions in different locations at the same time, these include the suprasellar, pineal and basal ganglia region. Other solitary locations of germinomas are the medulla oblongata, frontal lobe or in pontocerebellar angle (1, 4). Here we report on one case of multiple germinomas. CASE REPORT A 38 year-old male presented with worsening headache, vomiting and bilateral dimunition of visual acuity. On clinical examination we found a fully conscious patient, GCS 15 /15, with Parinaud syndrome. Fundus examination revealed papilledema. Visual field assessment showed an upward gaze deficit. Radiological findings on axial cuts of the Computed Tomographic Scan of the head and Brain Magnetic Resonance Imaging (MRI) showed multiple lesions in the pineal, suprasellar and at the right pontine cerebellar angle (PCA) with hydrocephalus (Fig1). A ventriculo peritoneal shunt was performed. No tissue biopsy was obtained. The analysis of Cerebro-Spinal Fluid (CSF) obtained during the ventriculo – peritoneal shunting showed the presence of tumor markers: alpha fetoprotein (αFP); and Human Chorionic Gonadotrophin (HCG). The patient then underwent radiotherapy and chemotherapy. The outcome was excellent with resolution of all the presenting symptoms and signs. The MRI done at the end of the cure revealed the remission of all the intracranial lesions (Fig2). DISCUSSION The development of the third ventricle leads to the displacement of the germ cell tumors outside the midline. The clinical manifestation of multiple germinomas depends on the location and size of the various tumors. Several clinical signs and symptoms are related to what is called cerebral hemiatrophy which is a result of lesions in the basal ganglia, thalamus, brainstem and cerebral hemisphere (1,4,5,7). The radiological findings in case of intracranial germinomas are as follows: Plain X-Ray of the skull may show a calcified mass in the pineal region. Head CT scan: the tumor usually appears as a circumscribed round or lobulated lesion, with iso- or hyperdense enhancement after contrast injection. On brain MRI the lesion is iso-intense on T1, iso or hyper intense on T2 with homogenous enhancement after gadolinium contrast injection (1,3,9) Hydrocephalus may be present because of the stenosis of the aqueduct of Sylvius near the pineal region. Tumors in the common location are often smaller than 60ml whereas the germinomas in atypical locations tend to be larger because of their high proliferation potential (8,9) If the tumor markers are positive then radiation and /or chemotherapy is indicated (1, 6,10) In our case ,we used both of them and our results were very good. Also in some cases ventriculo-peritoneal shunting is necessary to release ICP as it was performed in our case even though the risk of seeding of the peritoneum with tumor has been described in rare cases in the literature (8). CONCLUSION Germinomas are sensitive to radiotherapy and chemotherapy. The role of surgical treatment is still a matter of debate.
 FIGURE 2: MRI T1
Articles récents
Commentaires récents
Archives
CatégoriesMéta |

© 2002-2018 African Journal of Neurological Sciences.
All rights reserved. Terms of use.
Tous droits réservés. Termes d'Utilisation.
ISSN: 1992-2647