
|
|
|
INTRODUCTION L’aphasie est définie comme une perte partielle ou totale du langage consécutive à une lésion cérébrale siégeant dans l’hémisphère dominant, le plus souvent le gauche. Elle affecte l’expression orale, la compréhension, la lecture et l’écriture, sans altérer les capacités intellectuelles ou psychiques du patient. Après un AVC, l’aphasie constitue l’un des déficits neurologiques les plus fréquents et les plus invalidants, impactant fortement la qualité de vie des patients et de leurs proches. (3,4,8) La récupération de l’aphasie post-AVC est imprévisible, car elle dépend de multiples facteurs : caractéristiques cliniques de l’AVC, profil démographique, accès aux soins et surtout neuroplasticité cérébrale(9). L’orthophonie a montré un grand intérêt dans la prise en charge. Cependant dans les pays à ressources limités comme le nôtre, il existe un accès limité à ce type de rééducation.(16) De plus, peu d’études africaines se sont intéressées au pronostic des aphasies, d’où la pertinence de cette recherche dont l’objectif est de déterminer les éléments pronostics de récupération spontanée des aphasies post-AVC. METHOLOGIE Il s’est agi d’une étude prospective, descriptive et analytique réalisée sur six mois (avril–septembre 2022) dans les services de neurologie des CHU de Treichville et Cocody. Population :
Analyse statistique : Les données ont été analysées à l’aide du logiciel SPSS version 16.0. Une analyse univariée a permis de décrire les caractéristiques sociodémographiques et cliniques des patients. Les variables qualitatives ont été exprimées en effectifs et pourcentages et les variables quantitatives en moyenne ± écart-type. Une analyse bivariée a ensuite été réalisée afin d’étudier les facteurs associés à l’évolution de l’aphasie. Les comparaisons ont été réalisées à l’aide du test du χ² pour les variables qualitatives et du test de Student pour les variables quantitatives. Le seuil de significativité a été fixé à p < 0,05. Considérations éthiques : Le consentement libre et éclairé de chaque patient ou de son représentant légal a été préalablement obtenu. La confidentialité des données et l’anonymat des patients ont été assurés. Une autorisation des chefs de service de neurologie des CHU de Treichville et Cocody a été également obtenue avant de commencer l’étude. Seize patients dont 11 de sexe masculin (sex-ratio H/F = 2,2) ont été retenus pour cette étude. L’âge moyen était de 56 ans ± 13 ans avec des extrêmes de 35 et 76 ans. Après 3 mois d’évolution spontanée post-AVC, une amélioration du langage a été observée chez 15/16 patients. (Tableau I) 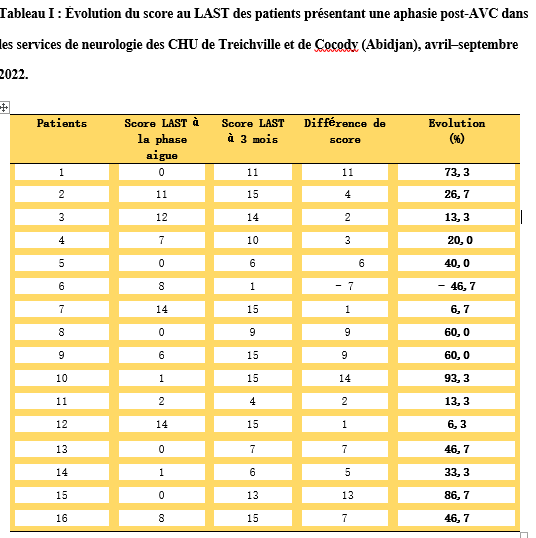 Le score total du LAST après 3 mois était significativement supérieur à celui de la phase aigüe (p =0,001). (Figure 1). 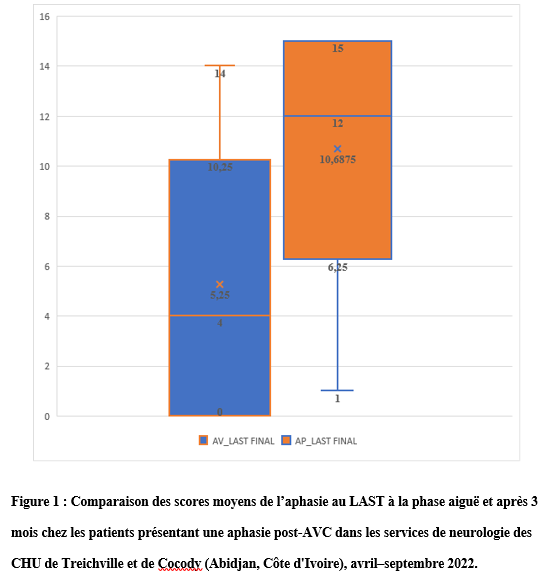 L’expression orale a évolué favorablement (p=0,008) notamment sur la dénomination (p=0,004) et la répétition (p=0,01) ainsi que la compréhension orale (p=0,02) portant sur ses différentes composantes (désignation, p=0,02 et exécution d’ordre, p=0,02). Par ailleurs, l’évolution semble meilleure chez les patients de sexe masculin (p=0,04), les non scolarisés (p=0,01), les hypertendus (p=0,04), les patients sans trouble de la conscience (p=0,01), ceux avec un score NIHSS sévère (p=0,02) et chez les patients victimes d’un AVC ischémique (p=0,02). En revanche, l’âge n’influençait pas significativement l’évolution. (Tableau II) 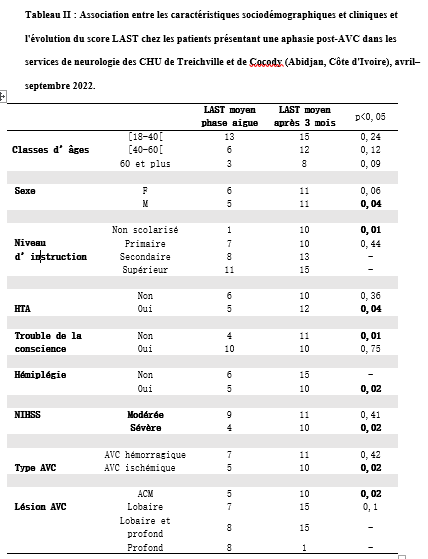 L’objectif de cette étude était de déterminer les facteurs pronostiques de la récupération spontanée des aphasies post-AVC après trois mois d’évolution. Les résultats montrent qu’une récupération spontanée du langage est observée chez la majorité des patients, avec une amélioration significative du score total au Language Screening Test (LAST). Par ailleurs, plusieurs caractéristiques sociodémographiques et cliniques, notamment le sexe masculin, l’absence de scolarisation, l’hypertension artérielle, l’absence de troubles de la conscience, un score NIHSS initial sévère et l’AVC ischémique, étaient associées à une meilleure récupération dans notre série. Nos résultats corroborent les données de la littérature concernant l’amélioration spontanée de l’aphasie au cours des trois premiers mois suivant un AVC, particulièrement au niveau de l’expression et de la compréhension orales. Cette évolution favorable témoigne des mécanismes de plasticité cérébrale qui caractérisent la phase précoce de récupération neurologique (6) Par ailleurs, la récupération du langage après un AVC chez les patients aphasiques dépend de multiples facteurs propres au patient et aux caractéristiques de l’AVC.(9) La récupération du langage après un AVC dépend toutefois de nombreux facteurs liés au patient et aux caractéristiques de la lésion cérébrale (10). Dans notre étude, les hommes présentaient une meilleure récupération langagière que les femmes. Ce résultat diffère des données de la littérature, qui rapportent essentiellement une association entre le sexe et le risque ou l’incidence de l’aphasie post-AVC, sans mettre clairement en évidence une influence sur la récupération elle-même.(5) Cette différence pourrait être liée à la faible taille de notre échantillon. Concernant la sévérité initiale, elle constitue classiquement l’un des principaux facteurs pronostiques. Or, contrairement aux grandes séries où un NIHSS sévère est plutôt un facteur de mauvais pronostic (1), notre étude a trouvé une évolution plus favorable dans ce groupe. Cette observation pourrait s’expliquer par un biais d’échantillonnage ou par une prise en charge hospitalière plus intensive et précoce des patients les plus sévèrement atteints. En outre, la topographie lésionnelle joue un rôle majeur. En effet, les atteintes limitées au territoire de l’artère cérébrale moyenne gauche, notamment frontales et temporales, sont associées à une meilleure récupération, comme le montre notre étude, tandis que les lésions corticales étendues ou profondes (capsule interne, thalamus) présentent un pronostic moins favorable. Ces observations sont concordantes avec celles rapportées dans la littérature (9) Concernant le niveau d’instruction, plusieurs études suggèrent qu’un niveau scolaire élevé favorise la récupération grâce à une meilleure réserve cognitive et à une plus grande plasticité cérébrale(7). A l’inverse, dans notre étude, les meilleurs résultats ont été observés chez les patients non scolarisés. Cette différence pourrait refléter le profil socioéconomique des patients hospitalisés dans les centres de santé publics. (2) Par ailleurs, la présence d’une hypertension artérielle (HTA) semblait contribuer à une meilleure récupération langagière. Alors que la littérature décrit généralement l’HTA comme un facteur péjoratif, probablement en raison de la microangiopathie chronique qu’elle induit (13). Ce paradoxe pourrait s’expliquer par un biais d’échantillonnage et par un meilleur suivi de ces patients, favorisant leur récupération fonctionnelle. Enfin, dans notre série, les patients ayant présenté un AVC ischémique ont montré une meilleure récupération langagière (p = 0,02) que ceux ayant un AVC hémorragique. Ce résultat est cohérent avec les observations de Seo KC et al., qui rapportaient une récupération fonctionnelle et cognitive plus favorable après un AVC ischémique. (10) Cette différence pourrait être liée à la persistance d’une zone de pénombre ischémique susceptible de favoriser les phénomènes de réorganisation cérébrale. En revanche, l’âge n’était pas significativement associé à la récupération dans notre étude, contrairement à certaines publications. Cette divergence pourrait s’expliquer par le faible effectif de notre série. De plus, la variabilité des outils d’évaluation (LAST, Boston Diagnostic Aphasia Examination, Western Aphasia Battery…) et des délais de suivi (deux semaines à plusieurs années) rend les comparaisons entre études parfois difficile [8;9;10]. Dans l’ensemble, nos résultats apportent des données préliminaires sur les facteurs associés à la récupération spontanée de l’aphasie post-AVC dans notre contexte. Toutefois, ces résultats doivent être interprétés avec prudence en raison du faible effectif de l’étude et de l’absence d’analyse multivariée, qui ne permettent pas d’identifier les facteurs pronostiques indépendants et limitent la généralisation des résultats. Des études multicentriques incluant un plus grand nombre de patients, un suivi prolongé et une analyse multivariée seraient nécessaires afin de confirmer ces observations et de mieux préciser les facteurs pronostiques de récupération de l’aphasie post-AVC. CONCLUSION Au terme de cette étude, une récupération spontanée significative du langage a été observée chez la majorité des patients présentant une aphasie post-AVC au cours des trois premiers mois d’évolution. Plusieurs caractéristiques sociodémographiques et cliniques étaient associées à une meilleure récupération dans notre série. Ces résultats contribuent à une meilleure connaissance du pronostic des aphasies post-AVC en Côte d’Ivoire. Toutefois, l’amélioration spontanée ne doit pas retarder la mise en œuvre d’une prise en charge orthophonique précoce, indispensable pour optimiser la récupération fonctionnelle et prendre en charge les déficits résiduels. DELAI D’ADMISSION DES PATIENTS VICTIMES D’ACCIDENTS VASCULAIRES CEREBRAUX ISCHEMIQUES A L’UNITE NEUROVASCULAIRE DU CENTRE HOSPITALIER UNIVERSITAIRE DE LIBREVILLE INTRODUCTION L’accident vasculaire cérébral ischémique (AVCI) correspond à un déficit neurologique de survenue brutale durant plus de 24 heures, secondaire à une diminution ou une interruption de l’apport sanguin cérébral, par oblitération artérielle ou trouble hémodynamique [25,8]. Il représente plus de 80 % des AVC [21,22] et constitue un problème majeur de santé publique en raison de sa mortalité élevée et des incapacités fonctionnelles qu’il engendre à long terme [11]. La physiopathologie de l’AVCI souligne l’importance cruciale du facteur temps : chaque minute de retard entraîne la perte d’environ deux millions de neurones et accélère le vieillissement cérébral, d’où le concept universellement admis de « Time is brain » [26]. La prise en charge précoce à la phase aiguë améliore significativement le pronostic fonctionnel et vital des patients. C’est dans ce contexte qu’ont été développées les unités neurovasculaires (UNV), reposant sur une prise en charge multidisciplinaire spécialisée. Les essais cliniques randomisés ont démontré que les UNV réduisent la mortalité, le handicap et le recours à l’institutionnalisation après AVC [27]. Ce bénéfice est renforcé par la thrombolyse intraveineuse (TIV), dont l’efficacité est étroitement dépendante du délai d’administration. Les recommandations de l’American Stroke Association préconisent un délai porte-aiguille (door-to-needle time) inférieur à 60 minutes [16,21], bien que seulement environ 30 % des patients atteignent cet objectif dans de nombreuses séries. Depuis octobre 2021, le Gabon dispose d’une UNV fonctionnelle au CHUL, avec accès à la thrombolyse intraveineuse. La présente étude avait pour objectif d’évaluer le délai d’admission des patients victimes d’AVCI dans cette unité et d’identifier les facteurs associés aux retards observés. METHODOLOGIE L’étude a été menée à l’UNV du service de neurologie du CHUL, ouverte depuis la mi-octobre 2021 et disposant d’une capacité d’accueil de cinq lits. Il s’agissait d’une étude transversale descriptive et analytique réalisée sur la première année de fonctionnement de l’UNV. Ont été inclus tous les patients âgés de 18 ans et plus, admis pour un AVC ischémique confirmé par l’imagerie cérébrale. Les données ont été recueillies à partir d’une revue documentaire des dossiers médicaux à l’aide d’une fiche d’enquête standardisée. Les variables étudiées concernaient les caractéristiques sociodémographiques, le jour et le lieu de survenue des symptômes, le mode de transport vers l’hôpital, les facteurs de risque cardiovasculaires, les données cliniques et paracliniques, ainsi que les modalités thérapeutiques. La variable dépendante était le délai d’admission à l’UNV, défini comme l’intervalle de temps entre la survenue des premiers symptômes et l’admission effective à l’UNV. L’analyse statistique a été réalisée à l’aide du logiciel Stata version 15. Les variables quantitatives étaient exprimées en moyenne ± écart-type ou en médiane avec intervalle interquartile selon la distribution. Les variables qualitatives étaient présentées en effectifs et pourcentages. Les variables ayant une valeur de p < 0,20 en analyse bivariée ont été introduites dans le modèle de régression logistique multivariée, afin d’identifier les facteurs indépendamment associés au retard d’admission. Le seuil de significativité était fixé à p < 0,05. L’anonymat et la confidentialité des données ont été strictement respectés. RESULTATS Au total, 146 dossiers de patients victimes d’AVCI ont été inclus durant la période d’étude. Les hommes représentaient 53,4 % de l’effectif, avec un sex-ratio de 1,1. L’âge moyen était de 58,9 ± 13,2 ans, avec des extrêmes allant de 24 à 88 ans. La majorité des patients vivaient en famille (94,9 %). Les retraités constituaient le groupe socioprofessionnel le plus représenté (41,1 %) (Tableau I). 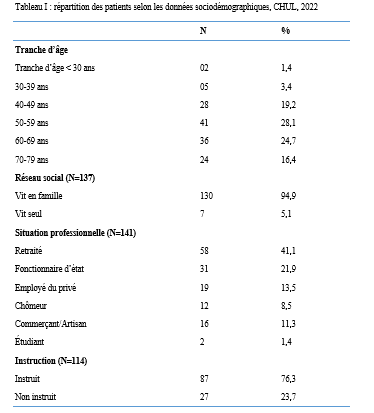 La distance médiane entre le lieu de survenue de l’AVC et le CHUL était de 6 km, et plus de la moitié des patients résidaient à moins de 10 km de l’hôpital. Les symptômes survenaient principalement à domicile (91,1 %) et en semaine (72,6 %). Une prise en charge non conventionnelle a été observée chez 18,5 % des patients, dont certains avaient eu recours à un tradipraticien. Le service d’appel des urgences n’a été sollicité que dans 3,4 % des cas. La majorité des patients (79,5 %) a été transportée au CHUL par un particulier. Le délai médian d’admission à l’UNV était de 11,5 heures, avec un délai moyen de 27,6 ± 54,7 heures. Plus de 75 % des patients ont été admis au-delà de la fenêtre thérapeutique de 4,5 heures. 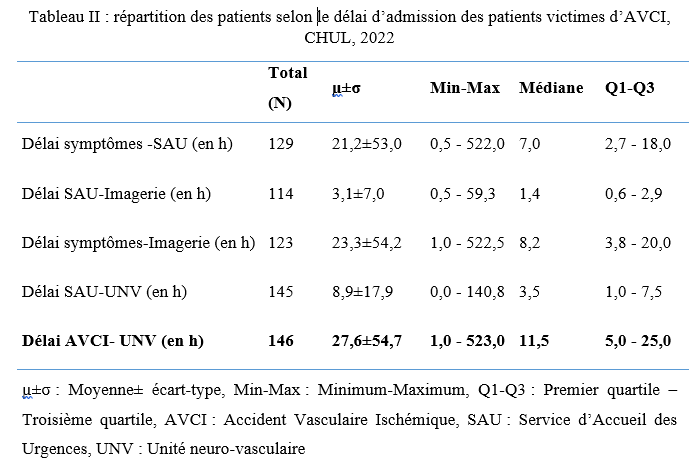 L’hypertension artérielle constituait le principal facteur de risque cardiovasculaire, retrouvée chez 72,6 % des patients. Le score de Glasgow moyen à l’admission était de 14,3 ± 1,6. Plus de 89% des patients présentaient un déficit moteur à l’admission à l’UNV. Les premiers symptômes étaient précisés chez 127 (87,0%) patients. Ils survenaient à domicile (91,1%) et en semaine chez 72,6% des patients. Par ailleurs, 27 (18,49%) patients ont eu une prise en charge non conventionnelle, parmi lesquels 15 patients ont eu recours à un tradipraticien. Le service d’appel des urgences a été contacté dans 3,4% des cas. Sur les 146 patients, 61 (41,8%) ont été pris en charge dans un autre centre avant d’être référés au CHUL. 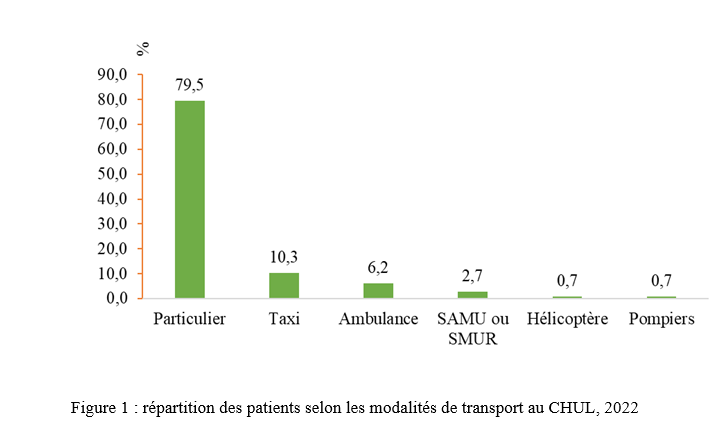 Les patients ont été conduits au CHUL dans 79,5% des cas par un particulier (figure 1) Sur l’ensemble des 146 patients inclus, 110 (75,3 %) ont été admis à l’UNV au-delà de 4,5 heures après l’apparition des premiers symptômes. En analyse bivariée, le retard d’admission à l’UNV était significativement associé à l’âge des patients (p = 0,043). Les patients âgés de moins de 50 ans présentaient un risque de retard d’admission trois fois plus élevé que ceux âgés de 50 ans et plus (OR = 3,1 ; IC95 % [1,0–9,6]). Les autres caractéristiques sociodémographiques, notamment le sexe, la situation matrimoniale, la profession, le réseau social, la distance par rapport au CHUL et le niveau d’instruction, n’étaient pas significativement associées au retard d’admission, bien que certaines tendances aient été observées (Tableau III). 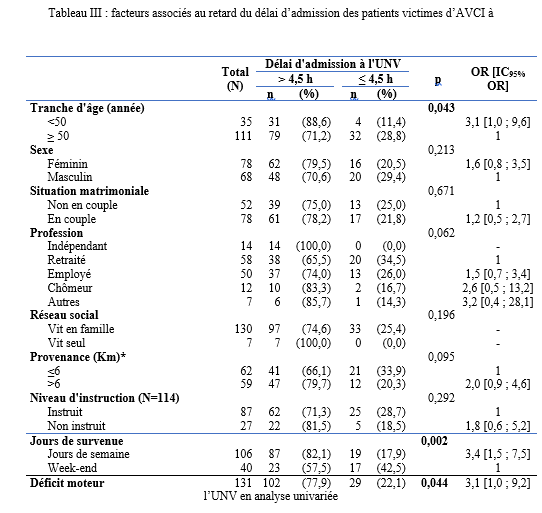 Par ailleurs, la survenue des symptômes en semaine était fortement associée au retard d’admission (p = 0,002), avec un risque multiplié par 3,4 (OR = 3,4 ; IC95 % [1,5–7,5]). De même, la présence d’un déficit moteur à l’admission était associée de façon significative au retard d’admission (p = 0,044), avec un OR de 3,1 (IC95 % [1,0–9,2]). Une fréquence élevée du retard d’admission était observée chez les femmes (79,5 %), chez les patients résidant à plus de 6 km du CHUL (79,7 %) et chez les patients non instruits (81,5 %), sans toutefois atteindre le seuil de significativité statistique. Après ajustement sur les facteurs de confusion potentiels, l’analyse multivariée a montré que deux variables restaient indépendamment associées au retard d’admission à l’UNV (Tableau IV). 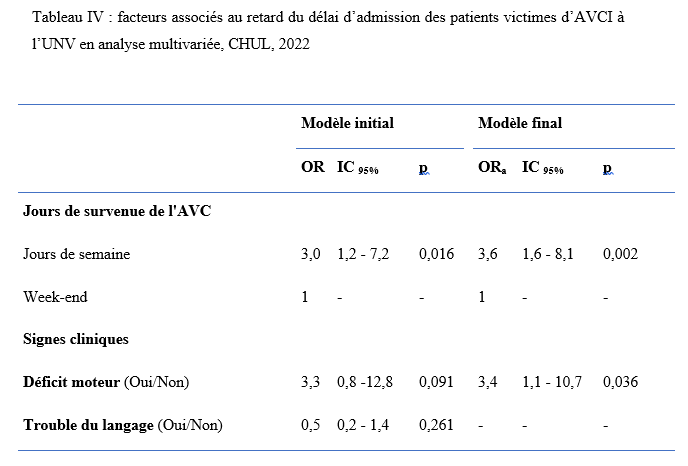 La survenue de l’AVC en semaine était associée à un risque significativement accru de retard d’admission (ORa = 3,6 ; IC95 % [1,6–8,1] ; p = 0,002). De même, la présence d’un déficit moteur à l’admission était un facteur indépendant de retard (ORa = 3,4 ; IC95 % [1,1–10,7] ; p = 0,036). Les troubles du langage n’étaient pas significativement associés au retard d’admission après ajustement. DISCUSSION L’accident vasculaire cérébral ischémique (AVCI) en phase aiguë constitue une urgence médicale absolue, nécessitant une prise en charge rapide et spécialisée dès les premières heures. Un diagnostic précoce et des interventions thérapeutiques appropriées améliorent significativement le pronostic vital et fonctionnel des patients. À l’inverse, un retard thérapeutique expose à des complications neurologiques sévères et engendre un coût économique important pour le patient, sa famille et le système de santé [22]. Dans notre étude, le délai moyen d’admission à l’UNV du CHUL après le début des symptômes était de 27,6 ± 54,7 heures, avec un délai médian de 11,5 heures. Près de 75,3 % des patients ont été admis au-delà de la fenêtre thérapeutique de 4,5 heures, limitant ainsi l’accès à la thrombolyse intraveineuse. Ces résultats sont comparables à ceux rapportés par Damon et al. au Sénégal en 2020, où le délai moyen d’admission des AVCI était de 26,59 ± 55,34 heures, avec seulement 33 % des patients admis dans les trois premières heures [10]. De manière générale, en Afrique subsaharienne, les délais d’admission demeurent largement supérieurs à la fenêtre thérapeutique recommandée pour la thrombolyse. Aref et al. en 2021 et Ahmed Nasreldein et al. en 2022 rapportaient respectivement des délais moyens de 8 heures et 12 heures [5,2]. Ces retards s’expliquent par des facteurs multiples, incluant des déterminants environnementaux, socioculturels et économiques. Comparativement, les délais observés dans notre étude sont nettement supérieurs à ceux rapportés dans les pays à revenu intermédiaire ou élevé. Ghadimi et al. en Iran en 2021 et Raúl Soto-Cámara et al. en Espagne en 2019 rapportaient des délais moyens et médians respectifs de 4,8 ± 5,7 heures et 2,2 heures [15,28]. Cette différence s’explique notamment par l’existence, dans ces pays, de filières de soins AVC bien structurées, incluant un « code AVC » activé dès la phase préhospitalière. En Iran, les patients dont les symptômes débutent dans les 4,5 heures sont intégrés dans un circuit de soins organisé permettant une prise en charge rapide. Des délais encore plus courts ont été rapportés en Italie par Vidale et al. en 2013, avec un délai médian de 2 heures [30]. En Suisse, Joachim Fladt et al. rapportaient en 2019 un délai préhospitalier médian de 3,1 heures, bien que près de la moitié des patients arrivaient encore au-delà de 4,5 heures, malgré un système de santé performant et une couverture géographique restreinte [14]. De même, en Europe et aux États-Unis, seulement un tiers des patients victimes d’AVC aigu arrivent à temps pour bénéficier d’une thrombolyse, malgré des systèmes de soins bien organisés [30]. Dans notre contexte, le retard préhospitalier observé pourrait s’expliquer par un faible niveau de sensibilisation de la population aux signes de l’AVC, mais également par l’influence persistante des mythes, croyances et représentations culturelles. Par ailleurs, le retard observé après l’arrivée à l’hôpital, notamment pour la réalisation et l’interprétation de l’imagerie cérébrale, suggère que la filière de soins AVC n’est pas encore pleinement optimisée. Or, les recommandations internationales préconisent un délai inférieur à 60 minutes entre l’arrivée à l’hôpital et l’initiation du traitement, incluant un délai d’interprétation de l’imagerie inférieur à 45 minutes [17]. Malgré les avancées majeures dans la prise en charge de l’AVCI aigu, les délais préhospitaliers n’ont pas significativement diminué depuis 2006 dans plusieurs pays, avec une majorité de patients n’arrivant pas avant trois heures [14]. Ces retards expliquent en grande partie la faible proportion de patients éligibles aux thérapies de recanalisation. Dans notre étude, les patients âgés de moins de 50 ans présentaient un retard d’admission plus fréquent que ceux âgés de 50 ans et plus. Ce constat rejoint celui de Tong et al. aux États-Unis en 2012, qui montraient que plus les patients étaient jeunes, plus le délai d’admission était long [29]. Cette situation pourrait s’expliquer par une moindre perception de la gravité des symptômes chez les sujets jeunes, souvent actifs professionnellement, retardant ainsi la recherche de soins. À l’inverse, les patients plus âgés, souvent entourés familialement et présentant davantage de comorbidités, perçoivent plus rapidement les symptômes comme graves. Une fréquence élevée de retard d’admission a également été observée chez les femmes (79,5 %), bien que le sexe féminin n’ait pas été significativement associé au retard. Amalia et al. en Indonésie en 2023 rapportaient toutefois une association entre le sexe féminin et la présentation tardive aux urgences [4]. Dans notre contexte, ce retard pourrait s’expliquer par la nature atypique ou non focale des symptômes. Une revue systématique et méta-analyse de Mariam Ali et al. en 2022 montrait que les femmes présentaient plus fréquemment des symptômes non focaux tels que la dysarthrie, les vertiges, les nausées ou vomissements, sources d’errance diagnostique, tandis que les hommes présentaient plus souvent des déficits focaux évidents [3]. Contrairement à d’autres contextes africains, la dépendance financière des femmes vis-à-vis de leur conjoint ne semble pas être un facteur déterminant au Gabon, où les femmes occupent une place socio-économique comparable à celle des hommes. Le niveau d’instruction n’était pas significativement associé au retard d’admission dans notre étude, bien que celui-ci soit plus fréquent chez les patients non instruits. Des observations similaires ont été faites par Kabanda et al. à Kinshasa en 2024. Un faible niveau d’éducation limite la reconnaissance des signes d’AVC et la compréhension de leur gravité, retardant ainsi le recours aux soins d’urgence [20]. Les antécédents cardiovasculaires, notamment l’hypertension artérielle et le diabète, étaient associés à une admission plus précoce, comme rapporté par Fladt et al. [14] et Kakame et al. à Kampala en 2023 [19]. Cette association pourrait refléter une meilleure sensibilisation de ces patients aux complications cardiovasculaires. Le retard d’admission était plus fréquent chez les patients résidant à plus de 6 km du CHUL, rejoignant les données montrant que l’éloignement géographique favorise le recours initial à la médecine traditionnelle, notamment en milieu rural [7]. Par ailleurs, les AVC survenus en semaine étaient associés à un risque de retard 3,4 fois plus élevé que ceux survenus le week-end, observation également rapportée par Damon et al. [9]. Ce phénomène pourrait s’expliquer par les contraintes professionnelles et la densité du trafic routier en semaine. Enfin, la majorité des patients (89,8 %) ont été transportés par des moyens non médicalisés. Des résultats similaires ont été rapportés au Gabon par Nyangui et al. [17] et au Togo par Balogou et al. [1]. Or, le transport médicalisé améliore significativement les chances de survie et de prise en charge précoce des patients victimes d’AVC [12]. La présence d’un déficit moteur était associée à un risque accru de retard d’admission, alors que la gravité globale de l’AVCI ne l’était pas. Ces résultats contrastent avec certaines études asiatiques et européennes, où la gravité des symptômes était associée à une arrivée précoce [6,13,18]. Dans notre contexte, le manque de reconnaissance des symptômes, l’automédication, le recours aux méthodes traditionnelles et la consultation initiale dans des structures non médicalisées pourraient expliquer ces observations. CONCLUSION Le délai d’admission des patients victimes d’AVCI à l’UNV du CHUL demeure long et largement supérieur à la fenêtre thérapeutique recommandée. Les principaux facteurs associés au retard d’admission étaient l’âge inférieur à 50 ans, la survenue de l’AVC en semaine et la présence d’un déficit moteur. Ces résultats soulignent la nécessité de renforcer la sensibilisation de la population aux signes de l’AVC et d’améliorer l’organisation de la filière de soins, notamment la phase préhospitalière et le transport médicalisé. Le développement d’un véritable « code AVC » et l’optimisation des délais intrahospitaliers constituent des perspectives essentielles pour améliorer le pronostic des patients victimes d’AVC au Gabon. TROUBLES DE LA DEGLUTITION POST-AVC : DETERMINATION DE LA LETALITE ET DES FACTEURS ASSOCIES A LEUR SURVENUE ET AU DECES AU CHU DE BRAZZAVILLE INTRODUCTION Les accidents vasculaires cérébraux (AVC) constituent une cause fréquente de handicap avec une altération significative de la qualité de vie (8, 12, 23). En Afrique subsaharienne, leur prévalence était estimée entre 15 et 770 pour 100 000 habitants en 2015 (2). Ils sont considérés comme la deuxième cause de mortalité après la cardiopathie ischémique et constituent un important facteur de risque pour les maladies cardiovasculaires. En tête de liste se trouvent les maladies infectieuses (22, 45). Au CHU de Brazzaville, les AVC constituaient la première cause de mortalité, soit entre 25 et 29% de décès ; la mise en place de l’unité AVC a permis de réduire la mortalité intrahospitalière de 30% (30). Des données récentes rapportent une mortalité intrahospitalière de l’ordre de 10,1 à 16,9% (31, 42). Les troubles de la déglutition (TD), constituent une complication fréquemment observée au cours des AVC. Ils intéressent près de la moitié des patients victimes d’AVC à la phase aiguë et sont associés à une morbimortalité élevée en l’absence d’une prise en charge adaptée et précoce (14, 18, 24). La présence de TD post-AVC est ainsi considérée comme un facteur de mauvais pronostic en raison de leur retentissement sur l’état nutritionnel, la fonction respiratoire et la prolongation de l’hospitalisation (15-17, 24, 39). Au CHU de Brazzaville, une fréquence de 26,9% a été retrouvée dans une publication portant sur le profil des TD post-AVC dans le service de neurologie (27). Les principales complications étaient la déshydratation (25,4%) et la malnutrition (10,2%), ainsi que la bronchopneumopathie d’inhalation (8,5%). A trois mois de suivi, 54,2% des patients étaient décédés ; en raison de la bronchopneumopathie et des fausses routes. La létalité en présence des TD ainsi que les facteurs associés à la survenue des TD et au décès n’avaient pas été abordés dans cette publication. La connaissance de ces données est déterminante pour une optimisation de la prise en charge des patients victimes d’AVC. L’objectif de cette étude de déterminer la létalité et les facteurs associés à la survenue et au décès des patients présentant des TD post-AVC en cours d’hospitalisation. Patients et méthodes Il s’agit d’une étude transversale, menée au CHU de Brazzaville dans le service de neurologie sur 6 mois. Avaient été inclus, tous les patients hospitalisés pour un AVC documenté par une imagerie encéphalique (TDM ou IRM), ayant donné leur consentement éclairé ou dont le consentement a été obtenu auprès d’un tiers informant. N’avaient pas été inclus, les patients présentant un score de Glasgow initial inférieur à 9, un antécédent de cancer ou de toute autre affection oto-rhino-laryngologique (ORL) pouvant être à l’origine des TD, ainsi que ceux présentant des TD secondaires à un AVC antérieur ou toute autre affection neurologique non vasculaire. La variable principale étudiée était la présence ou non de TD. Le dépistage des TD était effectué par la recherche systématique et quotidienne du réflexe nauséeux chez tous les patients par un étudiant en médecine, préparant une thèse d’exercice et formé à l’examen neurologique, sous la supervision directe d’un neurologue senior. Sa diminution ou son abolition indiquait la présence de TD, qui étaient confirmés systématiquement par le test 3Oz de DePippo (13). Les variables explicatives se rapportaient aux caractéristiques sociodémographiques, cliniques, paracliniques et thérapeutiques des patients, qui ont été pour certaines présentées dans une publication initiale (27). Analyse statistique L’analyse des données a été réalisée avec le SPSS 20.0. Les variables quantitatives ont été exprimées en moyenne ± écart-type et les variables catégorielles en effectif et pourcentage. La normalité de la distribution des variables quantitatives a été évaluée au préalable à l’aide du test de Shapiro-Wilk. Les variables explicatives, incluant l’âge (en années), associées à la survenue des TD et au décès en présence de TD ont été déterminées par une régression logistique simple, puis multiple ; dans laquelle les variables avec un p ≤ 20% ont été intégrées. La comparaison concernant l’issue hospitalière des patients avec et sans TD a été réalisée par le test exact de Fisher en raison des effectifs faibles. Le seuil de significativité était fixé à 5%. Clairance éthique et conflit d’intérêts Cette étude a été approuvée par le comité d’éthique pour la recherche en sciences de la santé (CERSSA) de l’université Marien Ngouabi. Les fiches d’enquête ont été anonymisées par un numéro d’identification codé afin de garantir la confidentialité des données. Un consentement éclairé, libre et écrit était obtenu auprès de chaque participant ou, en cas d’incapacité, auprès d’un tiers légalement autorisé. L’étude était conduite conformément aux principes éthiques de la Déclaration d’Helsinki. Les auteurs ne déclarent aucun conflit d’intérêt. RESULTATS Caractéristiques des patients Durant la période d’étude, 219 patients ont été admis pour un AVC, dont 136 (62,1%) hommes et 83 (37,9%) femmes, soit un sex-ratio hommes/femmes de 1,6. L’âge moyen des patients était de 63,41±14,24 ans [27-95 ans]. Les autres caractéristiques sociodémographiques sont présentées dans le tableau I. Un AVC ischémique a été objectivé chez 140 (63,9%) patients et un AVC hémorragique chez 79 (36,1%) patients. Fréquence des troubles de la déglutition Parmi les patients inclus dans l’étude, des TD ont été objectivés chez 59 (26,9%) d’entre eux. La répartition des patients selon la présence ou non de TD, par tranches d’âge et selon les caractéristiques sociodémographiques, est présentée respectivement sur la figure 1 et dans le tableau I. 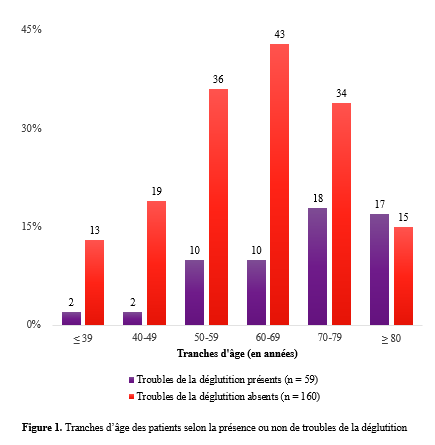 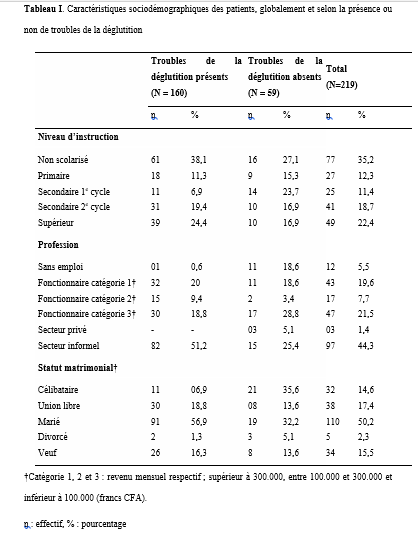 Le tableau II et la figure 2 présentent, respectivement, la localisation des AVC ischémiques et hémorragiques, selon la présence ou non de TD. 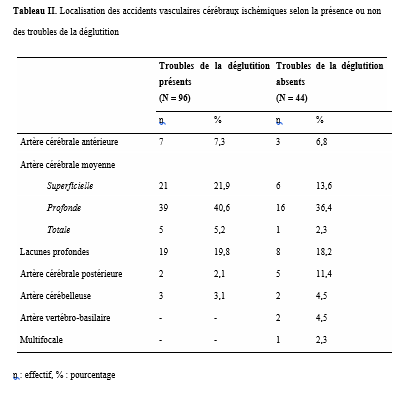 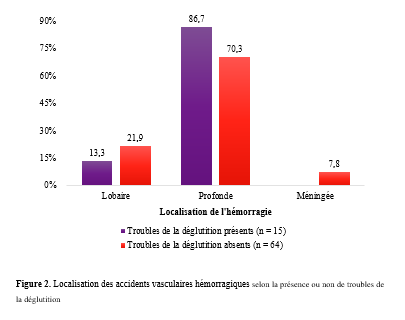 Facteurs associés à la survenue des troubles de la déglutition Le tableau III présente les résultats de l’analyse univariée par régression logistique des facteurs sociodémographiques, cliniques, paracliniques et thérapeutiques, associés aux TD. Après une régression logistique multiple, les facteurs associés aux TD dans le modèle final étaient la consommation d’alcool [ORa : 4,48 (1,69-11,84) ; p=0,002] et la présence d’une double atteinte pyramidale [ORa : 11,23 (4,68-26,96) ; p<0,001]. 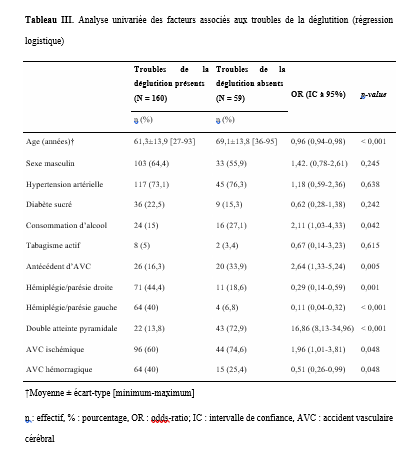 Décès et facteurs associés au décès en présence des troubles de la déglutition Durant l’hospitalisation, 22 (10%) patients sont décédés, dont 21 (95,4%) avec TD et un (4,5%) sans TD (test exact de Fisher, p<0,001). La létalité était de 35,6% parmi 59 les patients présentant des TD et de 0,6% parmi les 160 sans TD. Le tableau IV présente les résultats de l’analyse univariée par régression logistique des variables sociodémographiques, cliniques, paracliniques et thérapeutiques. Après une régression logistique multiple, dans le modèle final, seule l’absence d’antécédents d’AVC était associée à un risque moindre de décès [ORa : 0,28 (0,09-0,88) ; p=0,029]. 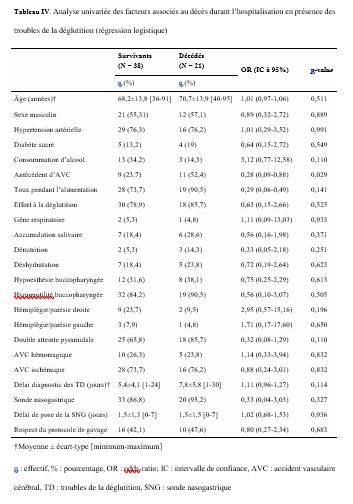 DISCUSSION Facteurs associés à la survenue des troubles de la déglutition Objectivés chez 26,9% des patients dans notre étude, les TD post-AVC sont fréquents au cours des AVC avec une fréquence d’environ 50% (3, 14, 24, 29). Nous avons retrouvé comme facteurs associés à leur survenue, la consommation d’alcool (ORa : 4,48) et la présence d’une double atteinte pyramidale (ORa : 11,23). La consommation d’alcool est l’un des principaux facteurs de risque d’AVC retrouvés au Congo-Brazzaville (5, 6, 42). Une consommation autodéclarée faible ou modérée réduirait le risque d’AVC, sans lien avec une variation génétique des gènes de métabolisation de l’alcool, ce qui laisse supposer qu’une consommation excessive augmenterait ce risque (7). La consommation d’alcool augmenterait également le risque d’hypertension artérielle et de cardiomyopathie dilatée non ischémique (32). En augmentant le risque d’AVC, la consommation d’alcool pourrait contribuer indirectement à la survenue des TD. Cependant, plusieurs autres hypothèses peuvent être émises, quant à son implication dans la survenue des TD post-AVC. Tout d’abord, la consommation d’alcool altère les fonctions frontales en réduisant la substance blanche sous-corticale frontale, du cervelet et du corps calleux, et en provoquant une perte neuronale au niveau du cortex préfrontal, de l’hypothalamus et du cervelet (35, 36). Lorsqu’elle est chronique et excessive, via une neuropathie alcoolique, elle peut réduire la pression du sphincter œsophagien inférieur et occasionner un reflux gastro-œsophagien, ou perturber le péristaltisme œsophagien à l’origine d’une dysphagie (28, 34). Ces altérations neurologiques peuvent affecter la déglutition, dont les troubles seraient potentialisés par la survenue d’un AVC. Par ailleurs, le sevrage alcoolique brutal imposé par l’AVC peut se compliquer d’une myélinolyse centro-pontine et extra-pontine due à un déséquilibre électrolytique, à l’origine d’un syndrome pseudobulbaire (33). Ce déséquilibre électrolytique pourrait également être accentué par l’hyponatrémie observée au cours des AVC dans le cadre du syndrome de perte de sel d’origine cérébrale (cerebral salt-wasting syndrome) ou de sécrétion inappropriée de l’hormone antidiurétique (37, 41). A ce titre, il conviendrait de mener une étude axée sur l’influence de l’alcool sur la survenue de TD post-AVC afin de mieux cerner son implication. La localisation de la lésion vasculaire est également incriminée dans les TD post-AVC. Le second facteur retrouvé dans notre étude était la double atteinte pyramidale, traduisant une atteinte hémisphérique bilatérale. Elle concernait 72,9% des patients présentant des TD, lesquels comptaient deux fois plus de récidives d’AVC. L’atteinte bilatérale du faisceau cortico-nucléaire peut se manifester par un syndrome pseudobulbaire, préférentiellement lors de lésions corticales (11, 24, 26). Cependant, des TD ont été également observés dans notre étude, chez des patients présentant un déficit moteur isolé de l’hémicorps droit et gauche, traduisant une atteinte hémisphérique unilatérale. Les muscles pharyngés et œsophagiens ont une distribution corticale asymétrique entre les deux hémisphères, d’où l’hypothèse d’un hémisphère de déglutition « dominant » (38, 43, 44). Par ailleurs, l’atteinte de certaines régions spécifiques peut également être à l’origine des TD par le biais des troubles de l’attention lors d’une lésion pariétotemporale ou de l’apraxie bucco-faciale lors d’une lésion pariétotemporale gauche (43). Les lésions de l’hémisphère gauche s’accompagnent d’une phase pré-pharyngée plus allongée due notamment aux difficultés d’initiation de la déglutition et celles de l’hémisphère droit, d’une dysfonction pharyngée, concernant les réponses automatiques et la coordination réflexe, plus sévère à la phase aiguë (9, 10, 20, 43). Décès et facteurs associés durant l’hospitalisation Bien que seuls 10% de nos patients soient décédés durant l’hospitalisation, principalement en raison de l’existence d’une unité AVC, 95,4% des décès concernaient les patients présentant des TD (p<0,001) (30). Selon Arnold et al. (3), le risque de décès demeure élevé jusqu’à 3 mois après l’AVC en présence de TD. Les TD post-AVC exposent à un risque nettement accru de décès, principalement en raison des complications respiratoires, notamment la pneumopathie d’inhalation, rapportée dans près de 20% des cas (3) et associée à un pronostic vital défavorable, particulièrement en cas d’aspiration (3 24, 40). En outre, la sous-estimation voire la méconnaissance des TD post-AVC pourraient retarder la mise en place de mesures préventives adéquates (14). La vidéofluoroscopie et/ou la nasofibroscopie représentent actuellement des outils complémentaires fiables pour l’évaluation des différentes phases de la déglutition, qui ne sont pas disponibles dans notre contexte d’exercice (19, 21). L’absence d’antécédents d’AVC était associée à un risque plus faible de décès en présence des TD (ORa : 0,28). Dans les lésions hémisphériques bilatérales, traduisant une potentielle récidive d’AVC sur l’hémisphère controlatéral, la récupération de la déglutition est plus lente, augurant un risque plus élevé de survenue de complications (20). Au Sénégal, 30,6% des décès liés aux AVC concernaient une récidive (25). En outre, la récidive d’AVC est associée à une mortalité plus importante notamment chez l’adulte jeune (1). Des thérapies de rééducation de la déglutition, comme la thérapie comportementale (exercices de rééducation, modifications alimentaires), l’électrostimulation neuromusculaire, la pharmacothérapie (anticholinestérasiques et agents prokinétiques) et la stimulation sensorielle, ont démontré leur bénéfice dans la réduction des complications nutritionnelles et respiratoires ainsi que sur l’amélioration des capacités de déglutition (4). Au Congo, le nombre insuffisant d’orthophonistes et l’absence de pratique de la gastrostomie et des thérapies spécifiques constituent des limites à la prise en charge optimale des TD post-AVC. Limites et forces de l’étude Cette étude présente certaines limites, notamment son caractères transversal et monocentrique, limitant la généralisation des résultats et l’inférence causale. Le dépistage initial des TD reposait sur la recherche du réflexe nauséeux, méthode peu sensible et peu spécifique, pouvant entraîner un biais de classification, malgré la confirmation par le test validé de DePippo. L’absence d’examens instrumentaux d’évaluation de la déglutition a pu conduire à une sous-estimation des dysphagies silencieuses. En revanche, cette étude présente plusieurs forces. Elle repose sur une population bien caractérisée, avec un diagnostic d’AVC confirmé par l’imagerie, et met en évidence des associations fortes et cliniquement pertinentes entre les TD, certains facteurs de risque (alcool, atteinte pyramidal bilatérale) et la mortalité. Elle apporte ainsi des données originales dans un contexte de ressources limités, soulignant l’importance du dépistage systématiques et précoce des TD comme levier majeur de réduction de la mortalité post-AVC. CONCLUSION Les troubles de la déglutition post-AVC sont à l’origine d’une mortalité considérable, réduite en l’absence d’antécédents d’AVC. La consommation d’alcool et une atteinte pyramidale bilatérale sont les facteurs associés à la survenue des troubles de la déglutition. Cependant, l’implication de l’alcool reste à préciser. La prévention primaire et secondaire des AVC ainsi que le dépistage systématique et précoce des troubles de la déglutition sont des mesures cruciales pour réduire l’incidence des AVC et initier des protocoles de prise en charge adaptés dans une approche multidisciplinaire intégrant des orthophonistes. MYASTHENIE ET SARCOÏDOSE : A PROPOS D’UN CAS ET REVUE DE LA LITTERATUREINTRODUCTION La myasthénie grave est une maladie auto-immune de la jonction neuromusculaire (8). Il s’agit d’une affection rare, dont la prévalence est estimée entre 45 et 142 cas pour 1 000 000 d’habitants. Elle peut survenir à tout âge, avec une nette prédominance féminine (6). Dans de rares cas, la myasthénie grave peut être associée à d’autres maladies auto-immunes telles que la thyroïdite de Hashimoto, le lupus érythémateux, la polyarthrite rhumatoïde ou le diabète juvénile (3). L’association entre la myasthénie grave et la sarcoïdose est encore plus exceptionnelle (4). Nous rapportons ici un cas illustrant cette association. OBSERVATION Monsieur XY, 29 ans, douanier de profession, a été reçu en consultation neurologique pour une vision dédoublée des objets surtout lors des contrôles de bagage sur l’écran du scanner, une modification du timbre de la voix ainsi qu’une faiblesse musculaire généralisée s’aggravant à l’effort. Cette consultation, effectuée le 29 décembre 2022, a permis de relever des épisodes rares de fausses routes ainsi qu’un ptosis en cas de fatigue extrême. L’examen clinique était normal. Le diagnostic de myasthénie grave a alors été envisagé. Un test à la prostigmine a été réalisé lors d’un épisode de fatigue associé à un ptosis, avec une régression marquée des signes. La recherche de l’anticorps anti-récepteur de l’acétylcholine (Ac anti-RACH) s’est révélée positive avec un titre de 0,8 nmol/ml (valeur normale < 0,2 nmol/ml). L’électromyogramme a montré une diminution modérée du potentiel moteur à la stimulation répétitive, de l’ordre de 9 %. Le scanner thoracique était revenu normal. Le patient a été mis sous pyridostigmine 60 mg comprimé à raison de un comprimé par 8 heures. L’évolution a été marquée par une régression des symptômes avec quelques épisodes de poussées. Trois ans plus tard, en Août 2025, le patient est revenu en consultation pour une dyspnée précédée depuis trois mois de toux sèche, résistante au traitement symptomatique ainsi qu’une fatigue survenant sans le moindre effort avec des épisodes de fièvre et de sueurs nocturnes. Une consultation pneumologique fut alors faite et permis de classer la dyspnée en stade 1 selon Sadoul. 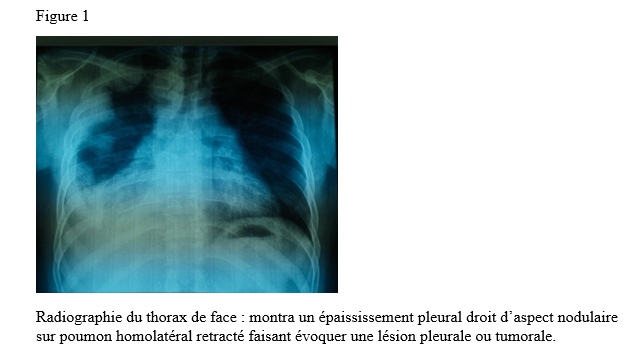 La radiographie pulmonaire de face (figure 1) montra un épaississement pleural droit d’aspect nodulaire sur poumon homolatéral retracté faisant évoquer une lésion pleurale ou tumorale. 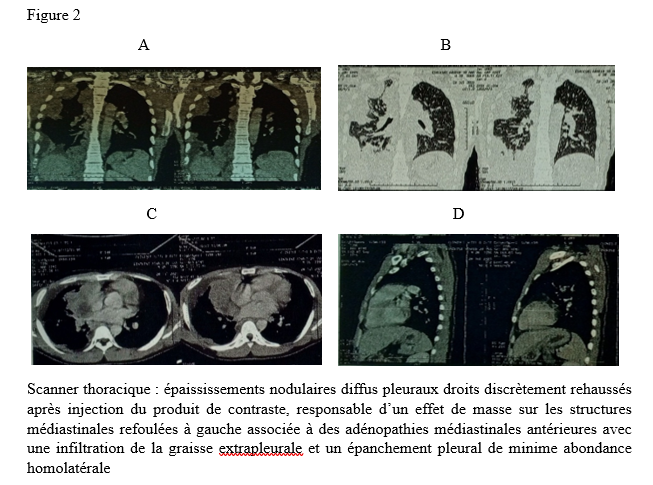 Le scanner thoracique demandé (figure 2) révéla des épaississements nodulaires diffus pleuraux droits discrètement rehaussés après injection du produit de contraste, responsable d’un effet de masse sur les structures médiastinales refoulées à gauche associée à des adénopathies médiastinales antérieures avec une infiltration de la graisse extrapleurale et un épanchement pleural de minime abondance homolatérale. Devant cet aspect scanographique, une fibroscopie bronchique fut réalisée montrant une muqueuse bronchique légèrement inflammatoire dans son ensemble avec épaississement des éperons de division entre la lobaire supérieur et moyen à droite et entre le culmen et la lingula à gauche siège de biopsie pour l’examen anatomo-pathologique sur les pièces ainsi que le genexpert du liquide broncho-alvéolaire. La recherche de tuberculose revint négative. 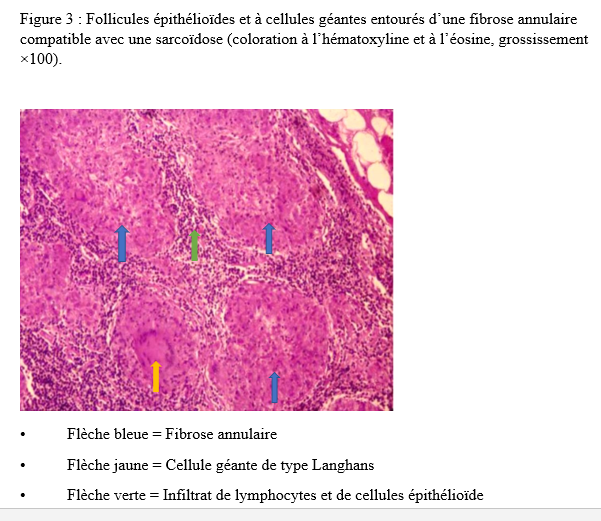 L’examen anatomo-pathologique des pièces biopsiques a permis de mettre en évidence la présence de granulomes épithélioïdes et giganto-cellulaires sans nécrose caséeuse (figure 3). L’examen de la peau et des phaners ainsi qu’une consultation ophtalmologique étaient normaux. La consultation rhumatologique était sans particularité. L’IRM cérébrale était normale. La spirométrie a révélé une CVF (FVCI) à 52 %, un VEMS (FEV1) à 63 %, VEMS/CVF> LIN avec absence de gain après bêta-2 mimétiques. Les données gazométriques étaient les suivantes : PaO₂ = 59 %, PaCO₂ = 54 %, pH = 7,39, Hb = 14,3 g/dl, HCO₃⁻ = 32 mmol/l. La calcémie était à 117mg/l ( 90-110 mg/l) l’IDR à la tuberculine est négative et le dosage de parathormone était revenu normal. Le diagnostic de sarcoïdose a été retenu chez notre patient. Un traitement par pyridostigmine 60 mg toutes les 8 heures et prednisolone à dose dégressive avec une dose d’entretien de 20 mg per os le matin au cours du repas a été instauré ainsi qu’un régime alimentaire pauvre en calcium et une exposition limitée au soleil. Ce traitement a permis une stabilisation de l’état clinique du patient sous surveillance multidisciplinaire. DISCUSSION Il est bien connu que des troubles de la réponse immunitaire peuvent coexister chez certains patients (12). Lorsque deux ou plusieurs maladies d’origine indéterminée sont retrouvées, plusieurs questions intéressantes se posent. Il est important de confirmer d’abord les diagnostics individuellement. Il est difficile d’aborder les mécanismes immunologiques qui déclenchent l’apparition de ces diagnostics ensemble. Bien que la coexistence de la MG et de la sarcoïdose puisse être une coïncidence, il convient de signaler ce cas en raison des multiples caractéristiques intéressantes observées ainsi que de la rareté de leur apparition. En effet, la survenue d’épisodes de fatigue chez un sujet myasthénique est souvent mise sur le compte d’une poussée myasthénique ce qui peut être source d’errance diagnostique. De même la survenue d’une hypercalcémie chez un sujet myasthénique peut orienter vers un trouble du métabolisme phospho-calcique en rapport avec une pathologie de la glande parathyroïde (13). Par ailleurs, la neurosarcoïdose est une complication chez 5 % des patients atteints de sarcoïdose (11). Les manifestations neurologiques les plus courantes de la sarcoïdose sont les neuropathies crâniennes dues à une méningite basale chronique. Le nerf facial est le plus souvent touché, parfois de manière bilatérale. Le nerf optique peut également être hypertrophié ou atrophié (2). L’examen ophtalmologique chez notre patient a révélé un fond d’œil normal ainsi que les nerfs oculomoteurs et il n’y avait aucun signe d’uvéite. Les autres nerfs crâniens étaient normaux aussi. L’IRM cérébrale n’a montré aucun signe de sarcoïdose. Toutes ces caractéristiques suggéraient la faible probabilité d’une neurosarcoïdose. Ainsi, l’hypercalcémie peut survenir dans les troubles formant un granulome tels que la sarcoïdose, en raison de la production rénale supplémentaire de 1,25-dihydroxyvitamine D. La libération de la PTH est inhibée par l’hypercalcémie et des niveaux élevés de calcitriol, ce qui explique la suppression du taux de PTH dans la sarcoïdose (5). Chez notre patient, le taux de PTH était normal, ce qui exclut une hyperparathyroïdie coexistante. La MG est une maladie auto-immune induite par l’apparition d’anticorps anti-acétylcholine Une dysrégulation des lymphocytes T est observée dans le sang périphérique (10). D’autre part, la sarcoïdose est une maladie systémique caractérisée par la formation de lésions granulomateuses à cellules épithélioïdes non accompagnées de nécrose, et sa pathogenèse n’est pas claire. Cependant, des informations récentes ont suggéré le mécanisme suivant de l’établissement des lésions granulomateuses des cellules épithélioïdes, bien que les détails soient encore inconnus (7). Les lymphocytes T sont activés après une stimulation non spécifique ou une stimulation en réponse immunitaire à une cause inconnue, et les lymphocytes T activés s’accumulent dans la lésion. Ces lymphocytes T accumulés produisent des lymphokines qui vont favoriser la différenciation des monocytes/macrophages en cellules épithélioïdes, ce qui entraîne la formation d’un granulome épithélioïde (7). Ceci parce que, le thymus joue un rôle important dans la différenciation et la croissance des lymphocytes T, on suppose que la MG en tant que « cause inconnue » active la lignée des lymphocytes T, induisant la formation de lésions de sarcoïdose. Toutefois, certains auteurs ont rapporté une sarcoïdose durant la période de rémission de la MG (1) d’autres une sarcoïdose pendant la période une poussée myasthénique (9) voire une régression de la MG et de la sarcoïdose après thymectomie (9). Le traitement de la myasthénie grave associée à la sarcoïdose repose en partie sur les mêmes molécules. Ainsi, notre patient a été mis sous anticholinestérasique (pyridostigmine), corticoïde (prednisolone). Nous sommes dans l’attente d’un avis spécialisé en immunologie, compétence qui fait actuellement défaut au Togo. CONCLUSION La myasthénie associée à la sarcoïdose est rare, mais doit être évoqué devant une myasthénie grave associée à des manifestations pulmonaires. Dans le contexte de la pandémie de VIH et de nouvelles pathologies émergentes en Afrique noire, il serait pertinent d’explorer systématiquement les liens possibles entre l’infection par le VIH ou des nouvelles pathologies, les infections pulmonaires associées et la survenue éventuelle de myasthénie grave associée à la sarcoïdose, afin d’optimiser la prise en charge des patients. LA NEUROPHOBIE CHEZ LES MÉDECINS URGENTISTES ET INTERNES AUX URGENCES MÉDICALES DANS LES HOPITAUX TERTIAIRES D’ABIDJAN EN 2024INTRODUCTION La neurophobie, ou crainte disproportionnée envers la neurologie, reste une problématique importante dans la formation médicale. Définie initialement par Jozefowicz, elle est liée à la complexité perçue des concepts neurologiques, à la difficulté des examens cliniques et au manque d’exposition pratique [4]. La littérature récente suggère qu’elle touche environ 30 % des étudiants en médecine, un tiers des médecins en début de carrière et des médecins généralistes [7]. En côte d’ivoire, la neurophobie concernait 27,4% des étudiants à Abidjan [5]. Ce phénomène, bien décrit chez les étudiants en médecine, pourrait également concerner les médecins urgentistes et internes, des acteurs clés dans la gestion des urgences médicales dans notre système de santé. Les urgences médicales constituent souvent le premier recours des patients souffrant d’affections neurologiques aiguës, nécessitant des décisions rapides et précises. Les services d’urgence (SU) dans le monde entier constituent un maillon vital entre la prise en charge pré hospitalière et l’hospitalisation des consultants [10]. Les médecins urgentistes et les internes des hôpitaux constitue le personnel médical de premier contact devant débuter en urgence la prise en charge des patients admis aux urgences médicales pour des affections neurologiques engageant le plus souvent le pronostic vital et fonctionnel des patients. Les urgences neurologiques constituent une activité conséquente dans les services d’urgences et les pathologies rencontrées sont très diverses et sont susceptibles d’entraîner une morbi-mortalité non négligeable si la prise en charge médicale n’est pas optimale dès les premières heures [6]. Selon l’OMS, les troubles neurologiques dépassent 6,3 % de la morbidité et 12 % de la mortalité dans le monde [9]. Ces chiffres ne feront qu’augmenter au fil des années [8]. La complexité décriée de la neurologie [2], pourrait de ce fait représenter un possible frein à la prise en charge optimale des patients avec des affections neurologiques. Forts de ce constat, nous avons réalisé ce travail dont l’objectif a été d’étudier la prévalence de la neurophobie chez les médecins urgentistes et internes aux urgences médicales des hôpitaux tertiaires d’Abidjan. MÉTHODOLOGIE
Il s’est agi d’une étude transversale menée sur une période de six mois allant de janvier à juin 2024. Nous avons réalisé un échantillonnage exhaustif auprès des médecins urgentistes et internes des hôpitaux qui ont assurés des astreintes et des gardes aux urgences médicales des CHU d’Abidjan. Les CHU de Cocody, de Treichville et d’Angré ont été les CHU de la ville d’Abidjan avec des urgences médicales fonctionnelles au cours de la période d’étude. La médecine d’urgence est une spécialité récente en Côte d’ivoire de ce fait elle est peu connue et donc il y’a peu de médecins spécialistes en la matière. Les urgences médicales fonctionnent avec plusieurs équipes médicales et paramédicales assurant les astreintes de jour et les gardes de nuit. Les internes des hôpitaux représentent encore les pierres angulaires sur lesquelles repose le fonctionnement des urgences médicales . Nous avons inclus dans notre travail, tous les médecins urgentistes et internes des hôpitaux pour qui un consentement été obtenu.
Les données ont été collectées via un questionnaire en ligne, conçu avec le logiciel Google Forms. Ce formulaire a été envoyé de façon individuelle et collective (plateforme d’échange Whatsapp), aux médecins urgentistes et aux internes des hôpitaux via l’application wathsapp. Nous avons recueilli les données socio démographiques (l’âge, le sexe, le nombre d’année d’expérience professionnelle) et l’évaluation de la neurophobie a été faite à l’aide du score neuroQ. Il s’agit d’un score validé pour apprécier la neurophobie [12]. Ce score repose sur 5 items (1- Je trouve que les concepts en neurologie sont difficiles à comprendre ; 2- J’ai confiance en ma capacité à comprendre la neurologie ; 3- En comparaison aux autres spécialités de médecine, je trouve que la neurologie est plus compliquée ; 4- J’ai confiance en ma capacité à étudier la neurologie ; 5- Je trouve qu’il est difficile d’appliquer les connaissances théoriques en neurologie à l’examen clinique du patient). Les réponses pour chaque item sont cotées de 1 à 5. Le score minimal est de 5 et le score maximal et de 25. Un sujet avec un score supérieur à 16 a été considéré comme neurophobe et un score supérieur à 18 a été qualifié de neurophobie sévère. Le questionnaire a été préalablement validé par les investigateurs. A partir du logiciel Google forms, les données ont été exportées et analysées sur Microsoft Excel. Pour les variables quantitatives, nous avons calculé des moyennes, des écarts-types et des intervalles de confiance. En ce qui concerne les variables qualitatives nous avons rapporté les fréquences. Les moyennes ont été comparées à l’aide du test de T-student. Considérations éthiques Les autorisations nécessaires auprès des autorités compétentes ont été obtenues avant la réalisation de l’étude. Les participants ont été informés de la nature de l’étude et ont donné leur consentement éclairé avant de remplir le questionnaire. L’anonymat et la confidentialité des répondants ont été strictement respectés tout au long du processus de collecte et d’analyse des données. RÉSULTATS Nous avons obtenu 59 réponses sur une population de 83 médecins internes et urgentistes aux urgences médicales sur notre période d’étude soit 71,08% de taux de réponses. Caractéristiques sociodémographiques La majorité des répondants étaitdes internes soit 51 sujets (86,44%), tandis que 8 (13,56 %) étaient des médecins urgentistes. L’âge moyen des participants était de 29,74 ans avec des extrêmes allant de 23 à 56 ans. Notre population d’étude a été constituée de 31 (52,54%) sujets de sexe masculin et de 28 (47,46%) sujet de sexe féminin. La moyenne du nombre d’années d’expérience professionnelle était de 3,27 (+/- 1,99) ans avec des extrêmes de 1 an à 10 ans. Plus de la moitié des sujets soit 53 (89,83%) avait moins de 5 années d’expérience professionnelle (figure 1). Prévalence de la neurophobie L’analyse du score de neuroQ a permis de retrouver 55 sujets non neurophobes soit 93,22% des cas (Tableau 1). Nous avons noté 4 sujets neurophobes (6,78%) parmi lesquels un seul avait une neurophobie marquée. Il n’y pas eu de différence statistiquement significative des moyennes des scores neuroQ entre les internes et les médecins urgentistes au seuil alpha de 5% (p=0,30). A la question de savoir pourquoi la neurologie était considérée comme une matière difficile, les principales raisons évoquées (figure 3) ont été : le besoin de connaitre la neuro anatomie (n=31) ; le besoin de connaitre la neurophysiologie (n=24) et le besoin d’être en situation pratique (n=21). Discussion Ampleur de la neurophobie Notre étude a permis de noté 6,78% de sujets neurophobes. Selon une revue systématique et méta-analyse de la littérature en 2024, la neurophobie est largement répandue chez les étudiants et les jeunes médecins, sa prévalence globale est estimée à 46% [3]. Dans une étude réalisée chez les médecins résidents aux urgences à Aragon, 27,6% [13] des médecins déclaraient souffrir de neurophobie. Cette différence de prévalence avec nos résultats pourrait être en lien avec les différences méthodologiques notamment sur les scores utilisés et sur la définition de la neurophobie selon les scores . Dans l’étude menée aux urgences d’Aragon, [13], en comparant la neurologie avec les autres spécialités, il était devenu évident que la neurologie se démarque de manière significative. Elle était perçue comme la discipline la plus difficile et c’était l’une des spécialités où ils se sentaient le plus incertains lors de la pose d’un diagnostic ou d’un examen physique [13]. Dans notre contexte de travail, peu d’études se sont intéressées à la neurophobie chez les étudiants en médecine, afin d’en apprécier l’évolution et les retentissements chez les médecins titulaires. Raison de la neurophobie Le besoin de connaitre la neuro anatomie; le besoin de connaitre la neurophysiologie et le besoin d’être en situation pratique ; ont été les principales raisons de la neurophobie dans notre travail. Cette étude représente la première étude réalisée sur la neurophobie chez les médecins aux urgences médicales en Côte d’ivoire. Une étude réalisée chez les étudiants en médecine à Abidjan a noté comme raisons principales de la neurophobie : le besoin de connaitre les bases des neurosciences, le besoin d’être en situation pratique et la complexité de l’examen clinique [5]. Bien vrai que la prévalence de la neurophobie soit plus faible dans notre étude, les raisons de celle-ci ne semblent pas différer de celles des autres études. Ainsi, dans l’étude réalisée chez les médecins urgentistes à Aragon [13] les principales raisons identifiées comme causes de leurs craintes et de leurs difficultés à l’égard de la neurologie étaient le type de patients et de diagnostic (62 ; 46 %), l’enseignement principalement théorique pendant leurs années universitaires (61 ; 46 %), suivi de la complexité des neurosciences fondamentales (physiologie, biologie et biochimie) (54 ; 40 %) et de l’exposition limitée aux patients neurologiques (49 ; 37 %). La revue systématique et méta-analyse de la littérature [3] avait noté en ce qui les raisons de la neurophobie, une association significative entre la difficulté et la complexité de la neuroanatomie, la nécessité de connaître les neurosciences de base, l’enseignement insuffisant et l’exposition limitée aux patients neurologiques. La prise en compte des raisons de la neurophobie devrait permettre aux systèmes éducatifs de mieux orienter le contenu et les axes de formation de la neurologie. Conséquence de la neurophobie Les cliniciens atteints de neurophobie peuvent se sentir mal à l’aise de gérer les maladies neurologiques, ce qui peut entraîner des références inutiles et des soins fragmentés pour les patients [11]. La neurophobie chez les médecins urgentistes et les internes des hôpitaux aux urgences médicales pourraient concourir à un retard ou un défaut de prise en charge en lien avec un défaut d’interprétation des symptômes et des signes présentés par les patients. Un autre effet indésirable de la neurophobie est celui de « trop de médicaments » associé à des examens paracliniques de plus en plus puissants mis au point pour le diagnostic d’affection neurologique. Ainsi, un manque de neurologues et une neurophobie de la part d’autres médecins, entraîneront une utilisation abusive et mal dirigée de ces examens paracliniques si les médecins ne sont pas correctement formés, en particulier dans les soins primaires [1]. Dans des pays avec des ressources limités et des populations avec des revenus faibles, l’accent devrait donc être mis sur l’amélioration de la formation aussi bien pré et post doctoral afin non seulement d’atténuer la neurophobie mais aussi, de limiter les dépenses liées aux soins et améliorer la prise en charge des patients. La neurophobie est un phénomène mondial qui influence les étudiants en médecine au cours de leur étude médicale mais aussi les médecins dans leur activité. Les patients de neurologie aux urgences posent le problème de pronostic vital nécessitant des prises de décision rapides . La neurophobie pourrait avoir un impact sur la prise en charge des patients aux urgences médicales présentant des affections neurologiques. La connaissance des facteurs incriminés de la neurophobie devrait permettre aux systèmes éducatifs d’élaborer des stratégies en vue de leur réduction. Conflit d’intérêt : les auteurs déclarent n’avoir aucun conflit d’intérêt. 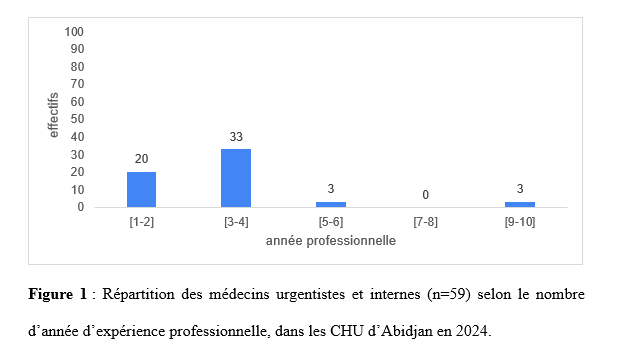 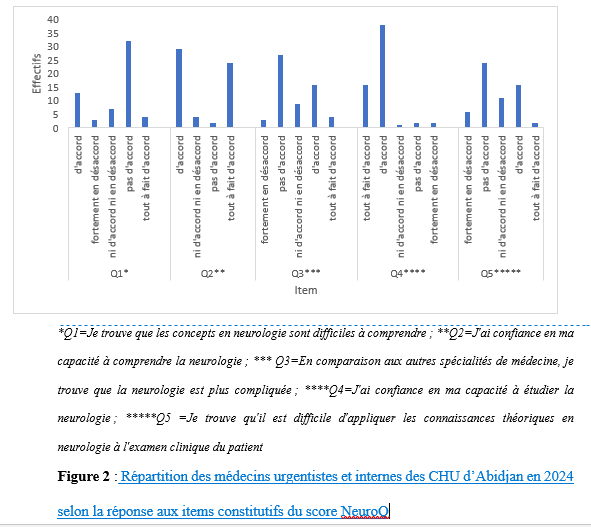 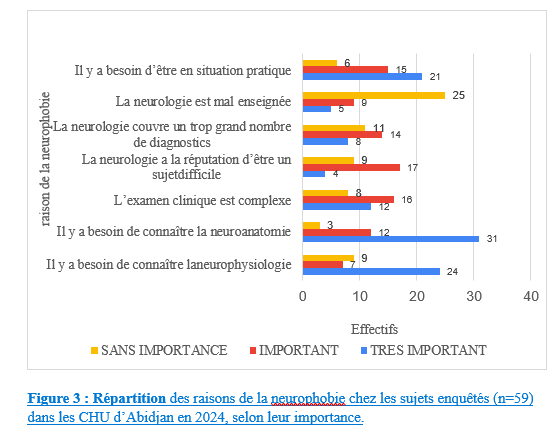 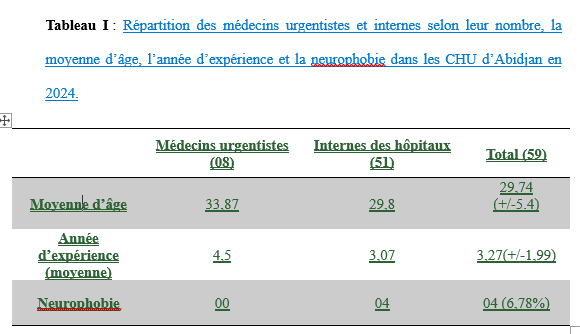 Articles récents
Commentaires récents
Archives
CatégoriesMéta |
© 2002-2018 African Journal of Neurological Sciences.
All rights reserved. Terms of use.
Tous droits réservés. Termes d'Utilisation.
ISSN: 1992-2647